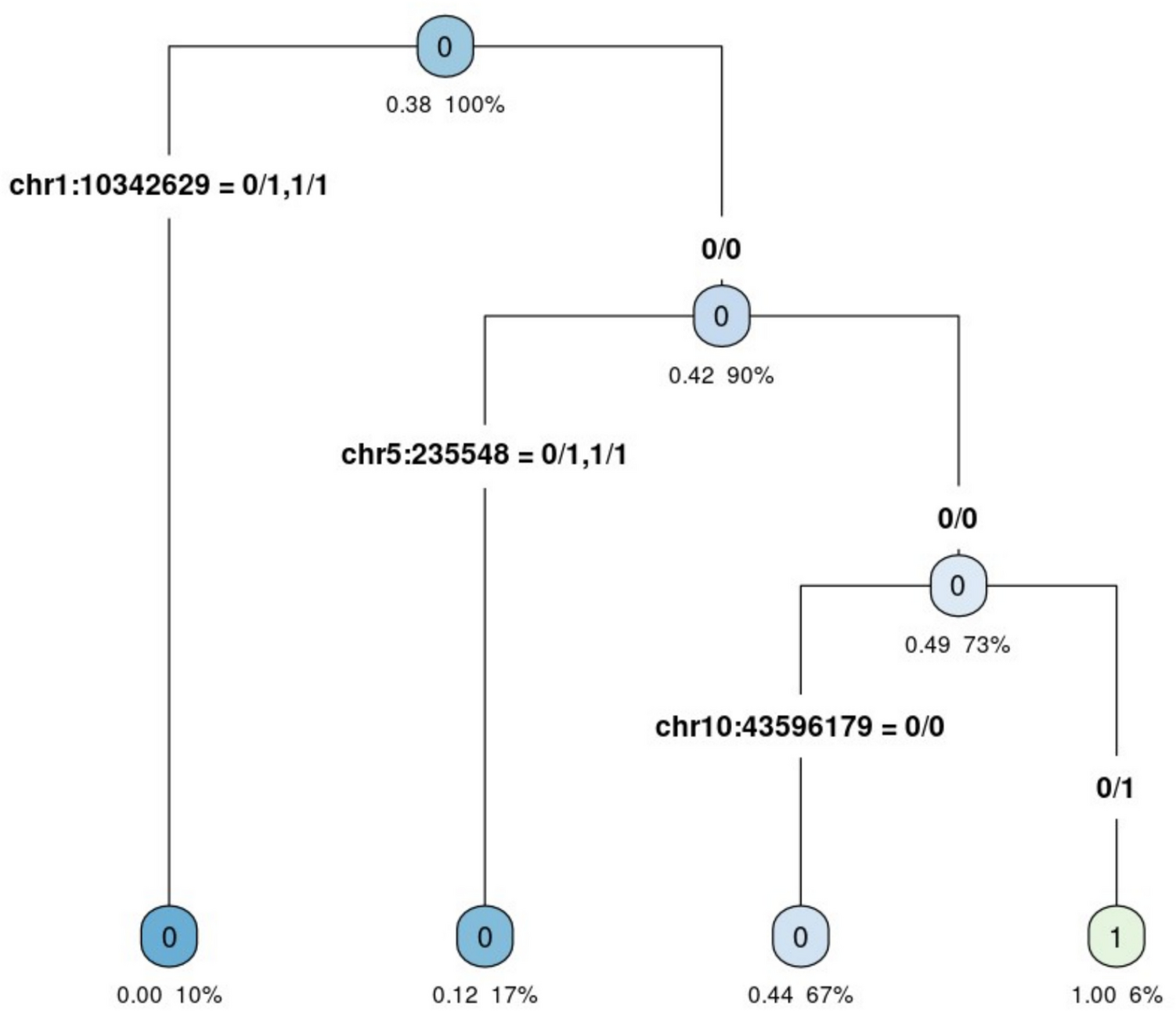
Paragangliomas can be caused by defects in various genes. Some of these defects are found to be common to different tumour sites (Katabathina et al. 2020; Calissendorff et al. 2022). Analysis of SNPs from the studied gene panel demonstrated that there are polymorphisms whose genotypes are indicative of tumour location. In particular, SNP rs3748576 (GA and AA genotypes) located on chromosome 1 within the KIF1B gene, as well as SNP rs10060259 (TC and CC genotypes) located on chromosome 5 within the SDHA gene, increase the probability of abdominal tumour locations, while heterozygous genotypes GA of SNP rs2435351 located on chromosome 10 within the RET gene increase the probability of head and neck locations. Although all three SNPs are located in introns and thus do not contribute to protein diversity, still, intronic SNPs can indirectly affect transcriptome diversity and expressivity by influencing alternative splicing (Bush et al. 2017) or stability of mRNA (Gupta et al. 2013), as well as overlap with non-coding RNA genes and other regulatory elements, especially enhancers that affect transcription (Lin et al. 2019). Moreover, the SNPs may be associated with the actual causal variants through strong linkage disequilibrium.
KIF1B (kinesin family member 1B) is a protein belonging to a family of kinesins involved in the transport of cellular materials to specified destinations (Hirokawa and Tanaka 2015). The family of these kinesins is involved in the morphogenesis, function, and survival of neuronal cells (Zhao et al. 2001). Mutations in the KIF1B gene in patients with PPGL have been described as germline and somatic. However, the potential importance of this gene in the development of these tumours remains elusive (Evenepoel et al. 2017). SDHA (succinate dehydrogenase complex flavoprotein A) is a subunit of succinate dehydrogenase (SDH), an enzyme that links two mitochondrial respiratory chain pathways: the Krebs cycle and oxidative phosphorylation. It is also one of the tumour suppressor genes (Gupta and Erickson 2023). Mutations in this gene have been described in patients with PGL with abdominal, cardiac, carotid body tumours, and in various other locations and origins, sympathetic or parasympathetic (Burnichon et al. 2010,Shi et al. 2023, Yoshihama et al. 2023, Nölting et al. 2022). Germline mutations in SDHA are described in approximately 10% of PPGL cases and have a low penetrance (Hanson et al. 2023). The polymorphism of the SDHA gene described in our study is located in intron 9 in a part of the gene that is close to the region coding the FAD binding domain that plays a role in maintaining the proper function of SDHA (Van Vranken et al. 2015). The RET (rearranged during transfection) protooncogene encodes a receptor tyrosine kinase, a membrane protein whose natural ligands are GDNF (glial-derived neurotrophic factor), neurturin, perception, and artemin. This protein controls the migration, survival, differentiation, proliferation, and maturation of vagal and sacral neural crest cells. Activation of receptor tyrosine kinase leads to the activation of numerous signalling pathways, including RAS/MAPK, PLCg, or PI3K (Bhattarai et al. 2022). RET germline mutations are detected primarily in patients with pheochromocytoma and much less frequently in those with paraganglioma (Currás-Freixes et al. 2015; Majewska et al. 2020). The detected polymorphism in the RET protooncogene was located in intron 2 of the gene and therefore was within the region associated with the coding sequences of the cadherin-like domains located in the extracellular part of the receptor kinase. Genetic defects in this region may lead to impaired expression of RET on the cell surface (Takahashi et al. 2020).
The PGLs of the head and neck and the PGLs of the upper mediastinum are mainly associated with the parasympathetic system and are not hormonally active. In rare situations (5%), catecholamine-secreting head and neck PGLs that arise from either the carotid body or the carotid sympathetic chain can be identified. PGLs that develop in the lower mediastinum, abdomen, and pelvis are associated with the sympathetic nervous system and are usually hormonally active (Choi et al. 2020). In our study, we dealt with head and neck tumours, which were unknown whether they were hormonally active before surgery. However, their location indicated a high degree of probability of parasympathetic origin. Therefore, it can be assumed that these two distinguished classes, 0 and 1, represented sympathetic (abdominal PGLs) and parasympathetic (head and neck PGLs) tumours, respectively.
From a bioinformatics perspective, the major limitation of the analysis was a small study population that impedes formal significance testing of individual variants. Moreover, a small sample size contributes to a low power of causal variants detection, which typically reveal low genotype variation and may not even be polymorphic in the analysed sample. Furthermore, the group of patients with PGLs of the head and neck was almost half as numerous as those with PGL of the abdomen. Another limitation is the lack of data on the hormonal activity of tumours located in the head and neck area.



Comments (0)