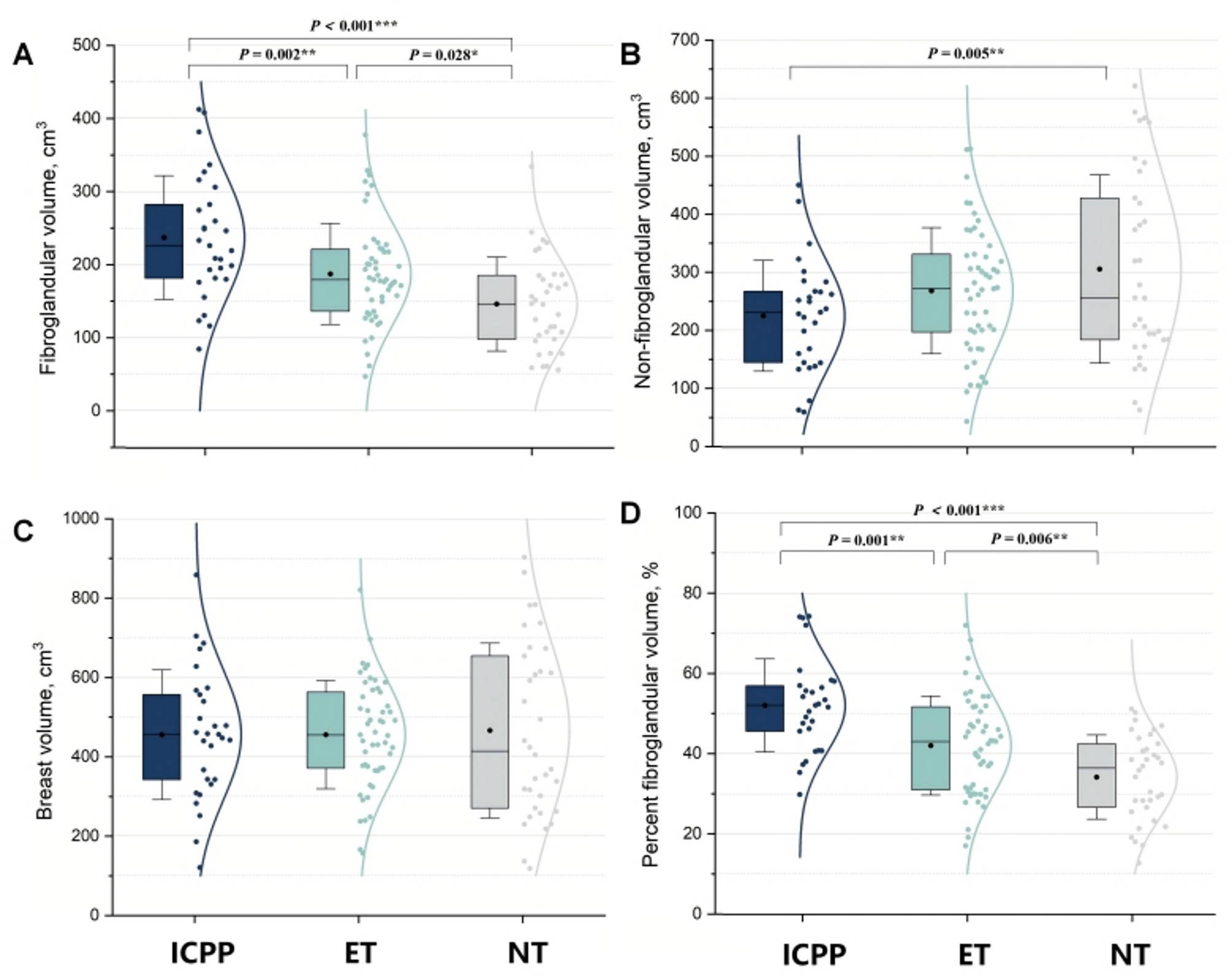
This is the first prospective study in girls to examine the association between earlier thelarche (onset before age 9) and MRI-based breast density—a well-established breast cancer risk factor—while also exploring the mediating role of reproductive hormone levels. Our findings show that each one-year earlier onset of thelarche was associated with a 35.7 cm³ increase in fibroglandular volume (FGV) and a 7.8% increase in percent FGV (%FGV). Notably, girls who experienced thelarche before age 8, as well as those between 8.0 and 9.0 years, exhibited significantly higher %FGV and FGV one year post-menarche compared to those with thelarche onset after age 9. These findings indicate that earlier thelarche, even within the clinically normal range and without meeting criteria for precocious puberty, is linked to substantially greater breast density.
Both baseline and follow-up estrogen levels mediated the association between earlier thelarche and increased breast density, with baseline levels showing a stronger mediating effect. In stratified analyses restricted to participants with consistently elevated estradiol levels (either at baseline or follow-up), girls with thelarche before age 9 had significantly higher FGV values than those with later thelarche onset.
Compared with the GOCS cohort, our study reported generally similar FGV, %FGV, and BV values [8]. However, as nearly one-third of the children in our cohort had ICPP, the values observed in participants with comparable ages at breast development were consequently lower than those reported in the GOCS cohort. The use of MRI in our study—recognized for its superior accuracy in assessing breast tissue composition—instead of DXA as used in GOCS, may account for some differences [22, 23]. Moreover, the higher prevalence of childhood obesity in the Western population [24], compared to Chinese children, may also contribute, given the influence of adiposity on breast development and volume.
The relationship between early thelarche and breast density remains insufficiently characterized. To date, only one prospective study—the Dietary Intervention Study in Children (DISC)—has examined this association, reporting a significant link between early thelarche and adult breast density after adjusting for BMI [9]. However, the findings from this study may not accurately reflect the effects of truly early thelarche, as the DISC cohort had a mean thelarche age of 10.6 years, with fewer than 5% of participants experiencing onset before age 9. More critically, DISC measured breast density in adulthood (mean age 27.2 years), by which time nearly one-third of participants had undergone pregnancy. Given pregnancy’s known transformative effects on breast tissue [15], adult assessments may mask thelarche’s direct biological influence.
Our prospective adolescent cohort study addresses these limitations by evaluating breast development during its dynamic, pre-pregnancy phase. Notably, over half of the participants in our cohort experienced thelarche before age 9, allowing for more robust assessment of early onset. The strong associations we observed suggest that previous research may have systematically underestimated the impact of early thelarche on breast density.
In our study, estrogen levels were positively associated with breast density, a finding consistent with several reports in perimenopausal women [25,26,27]. However, other studies have reported either inverse or null associations between estrogen and breast density in middle-aged and older women [28, 29]. Among adolescents, exogenous estrogen exposure between ages 12 and 17 has been linked to higher adult breast density [16]. Elevated IGF-1 levels during adolescence have also been associated with increased breast cancer risk [30]. In contrast, studies in young adult women have found no significant association between circulating estrogen and breast density [31]. These inconsistencies may reflect the dynamic and stage-dependent effects of reproductive hormones on breast tissue across the female lifespan. In supplementary analyses, we examined the association between circulating androgens and breast density; these analyses did not reveal a significant relationship. This lack of association may reflect an age-specific effect of androgens, whose influence on breast cancer risk has been primarily documented in adults and may not extend to children [32,33,34]. Further studies are warranted to investigate this potential relationship more comprehensively across different developmental stages. Therefore, interpreting the relationship between reproductive hormones and breast density requires careful consideration of population characteristics and developmental timing. As current evidence is largely derived from adult populations, further studies in adolescent cohorts are needed to clarify these associations.
Although prior research has proved the complex association between reproductive hormones and breast density, their role in the association between early puberty and breast density remains unexamined. While estradiol, IGF-1, and progesterone are well-established regulators of pubertal mammary development [15], their role in mediating the relationship between earlier thelarche (< 9 years) and breast density had not been previously investigated. Our mediation analysis demonstrates that these hormones collectively account for 28.7% of this association, with estradiol exhibiting the most pronounced mediating effect. This hierarchical pattern—where estrogen’s influence surpasses that of IGF-1 and progesterone—aligns with existing models of estrogen receptor-driven mammary proliferation [35, 36]. These findings suggest that earlier thelarche may trigger enduring morphological changes through endocrine programming, potentially establishing lifelong trajectories of breast cancer risk.
In recent years, the incidence of breast cancer has shown a steady increase with a concerning trend toward younger age at diagnosis [37, 38], underscoring the critical need to identify early risk factors and explore potential preventive interventions. Prior epidemiological studies have established an association between earlier age at menarche and increased breast cancer risk; since early thelarche typically precedes and contributes to early menarche, the onset age of breast development may represent a more proximal and biologically significant exposure in breast carcinogenesis. Evidence from retrospective studies, including the UK Breakthrough Generations Study and the US Sister Study, suggests that earlier thelarche is associated with a 20–30% increased risk of breast cancer later in life [6, 7]. The secular trend toward earlier thelarche - advancing at 0.25 years/decade worldwide [4] - exhibits disturbing synchrony with two key epidemiological shifts: rising breast cancer incidence and younger age at diagnosis. This temporal synchrony provides compelling evidence that pubertal timing plays a causative role in breast carcinogenesis, establishing thelarche not only as a biological milestone but also as a promising target for preventive interventions.
Our findings demonstrate that estrogen levels during thelarche onset serve as a key mediator linking earlier puberty to increased breast density. This observation aligns with established evidence from middle-aged and older women, where elevated circulating estrogen concentrations are positively associated with breast cancer incidence [39, 40]. These results provide empirical support for the mechanistic hypothesis that earlier estrogen exposure during puberty induces persistent morphological changes in breast tissue, potentially increasing lifetime breast cancer risk [6]. The clinical implications of these findings are that they identify peripubertal estrogen exposure as a modifiable factor influencing breast density. These insights may inform future strategies for breast cancer risk reduction, particularly in populations experiencing earlier pubertal timing.
While age at menarche is routinely documented in epidemiological studies, thelarche timing remains significantly underreported. Future research should prioritize standardized assessment of thelarche onset to better elucidate its independent association with breast cancer risk and evaluate its potential for improving existing risk prediction models. The incorporation of this metric into clinical practice could facilitate earlier identification of high-risk individuals who might benefit from personalized screening approaches or targeted preventive strategies. Although additional longitudinal investigations are required to establish causal relationships, our findings provide compelling biological evidence supporting exploration of puberty-delaying interventions in high-risk populations (particularly girls with familial breast cancer predisposition) and highlight the clinical value of incorporating endocrine marker monitoring into routine adolescent health evaluations.
This study has several notable strengths. To our knowledge, it represents the first longitudinal investigation examining the association between early thelarche and breast density in adolescents, featuring serial hormonal profile assessments at two critical developmental time points. The study’s limitations include a relatively small sample size which, while sufficient for initial hypothesis testing, may constrain statistical power for subgroup analyses and limit generalizability to broader populations. However, this limitation is partially mitigated by the deliberate inclusion of participants spanning the full continuum of normal and precocious puberty, ensuring adequate phenotypic variability.
Another limitation is that breast density assessments were conducted at an average age of 12 years, when breast development was ongoing rather than complete. At the time of imaging, the majority of participants had reached Tanner stage 5, but not all, indicating some variability in developmental status. Although this precludes definitive conclusions about final adult breast density patterns, the ongoing follow-up of this cohort will enable future evaluations at later developmental stages, providing valuable insights into long-term density trajectories in girls with early puberty. Finally, as with all observational studies, residual confounding by unmeasured environmental or genetic factors cannot be entirely ruled out. Nevertheless, the consistency of our findings with established biological mechanisms and prior epidemiological evidence lends credibility to our conclusions. Future studies with larger samples, more frequent assessments, and extended follow-up into adulthood will be essential to validate and expand upon these important preliminary findings.




Comments (0)