Diagnostic branched tree assessment is a method used to evaluate a learner’s clinical reasoning by guiding them through a series of branching decisions that simulate the diagnostic process. Each decision point represents a choice based on patient information, where the learner must select the most appropriate next step. This approach is useful because it mirrors real-world diagnostic decision-making and can reveal not only the final diagnosis but also the reasoning process behind it. Choose Your Own Adventure (CYOA)-style assessments build upon DBT by increasing the number of options at each decision point, offering a more complex and nuanced exploration of clinical reasoning. Learners enjoy the CYOA assessments, and participation in this type of activity increases academic performance and engagement [31].
In this study, we developed a tool that takes data from CYOA case studies to generate maps that reflect clinical reasoning. These maps clearly illustrate the range of possible pathways within each case study and reveal patterns in decision-making. Trends, such as the proportion of users taking a particular path or the nodes where users diverge from the expert path, were easily identifiable. These data visualizations also provide a straightforward approach to compare two different approaches to a clinical problem. Traditionally, this type of data is presented in cumbersome tables, but our tool provides assessors with an intuitive, scalable graphic representation of user behavior. Data visualizations have been increasingly used across medical education and practice to facilitate understanding and improve outcomes. Mapping tools have been designed to identify gaps and redundancies within courses [32, 33] and to serve as dashboards for student learning [34]. The shared goal for these tools is to quickly disseminate information, reduce errors, streamline data interpretation, and improve outcomes, whether for students or patients. By tracing user behavior, the CYOA mapping tool revealed the structure and flow of clinical decision-making, supporting its value as a dynamic data visualization instrument.
To our knowledge, this study is the first to incorporate data visualizations with CYOA assessments to reveal decision-making patterns in complex clinical case studies. While CYOA assessments have been used in several medical education contexts [17, 22,23,24,25,26], this is the only study that has incorporated a data visualization of the CYOA map and user behavior. The integration of visual tools into CYOA-style assessments offers a powerful way to streamline the evaluation of complex decision-making processes and foster deeper clinical reasoning skills. The strength of this study lies in its ability to display numerous potential treatment pathways, including routes that diverge from and rejoin the expert path. This mimics the choice architecture inherent in clinical decision-making and supports the view that there is rarely only one “right” way to diagnose or treat a patient [11]. This approach contrasts with traditional assessments like multiple-choice questions, which tend to favor a single correct answer [5]. In clinical practice, physicians must tolerate uncertainty [35], and assessments promoting only one correct answer may inadvertently discourage flexibility. By incorporating CYOA assessments as formative tools with instructor coaching [2, 36], students can be exposed to a range of acceptable decision-making pathways and develop a tolerance for ambiguity, a critical skill in clinical practice [37, 38].
Building on this idea, our approach offers intriguing opportunities for both developing and assessing learning outcomes going forward, especially as it pertains to case-based learning (CBL). CBL discussions are typically led by a clinical instructor who prompts students to engage in clinical reasoning. Work by Gartmeier et al. [39] showed that most questions posed by clinical instructors in case-based learning scenarios are initial, rather than follow-up, and close-ended rather than open-ended. This creates a challenge for ensuring that CBLs encourage the development of deep clinical reasoning. Follow-up questions push students to view decision-making as an evolving process rather than a means to reach a single pre-defined conclusion. We envision this system being used in future applications as a formative assessment tool that promotes discussion of open-ended, reasoning-based questions. For example, while this pilot study mapped cohort-level progress through case studies, future iterations could be used in active-learning classrooms, where students complete a case study at the beginning of class and then analyze decision-making pathways, reflect on clinical reasoning strategies, and link the study back to the learning objectives of the unit. Using the map of user behavior, instructors could give targeted feedback on common decision-making pitfalls and reinforcement of expert reasoning strategies. This method could also easily be adapted for use in a flipped classroom: learners could complete the CYOA case study outside of class, and in-class sessions would be centered around the analysis of the CYOA map. Overall, the tool could help correct misconceptions, build new knowledge, and foster critical thinking in many medical education settings.
Future research will focus on how this tool can be operationalized in the classroom, exploring both learner and instructor attitudes toward its use. Another avenue for future exploration is applying this methodology to other domains that require dynamic and longitudinal patient management. Further refinement of the system will aim to determine the most effective ways to display decision-making maps for rapid evaluation [40] and optimize the number of options and branches within each decision point [27].
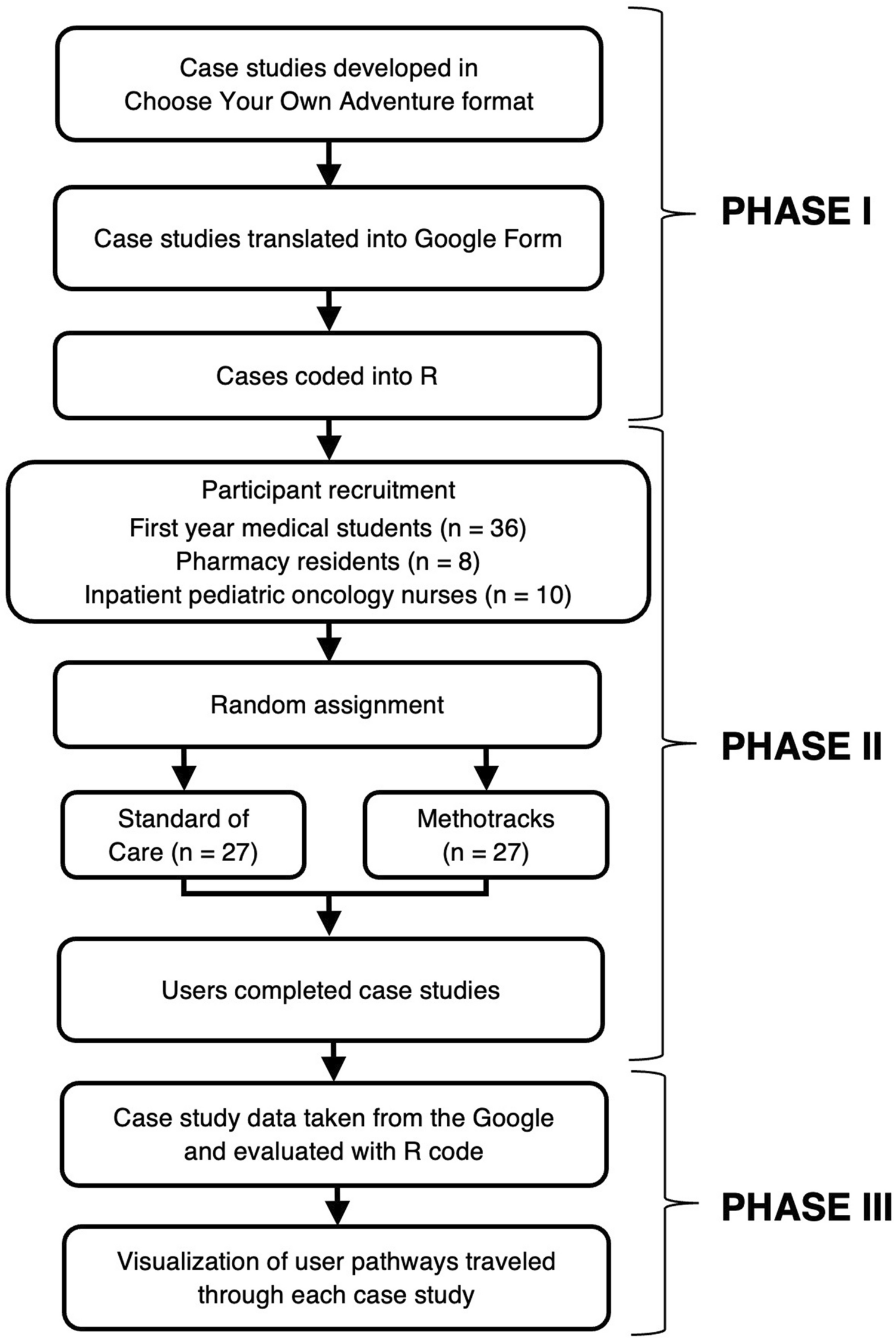
There were several limitations to this study. One major limitation was the small sample size and restriction to a single university, which may have influenced the pathways chosen by users. These choices could reflect a lack of familiarity with Methotracks or therapeutic management rather than true decision-making behaviors. Furthermore, the CYOA case study used in this study was administered through Google Forms which has a “go back” button that cannot be disabled. For this reason, we opted to blind users from the outcome of their treatment decision. While this decision gave us a more honest look at how users were traversing the case study, it limited our ability to gather insights into how users reflected on their decision-making process. Future iterations of this study will incorporate these changes to better understand how this system could be used in a classroom environment. A final limitation is the time-intensive nature of creating DBT and CYOA case studies, which require authors to account for multiple pathways and endings. The creation of the accompanying maps also requires proficiency in R-based coding.
Despite these challenges, the potential for DBT and CYOA assessments to more closely mimic real-world decision-making is high [22].Therefore, the issue becomes how to make these types of cases easier to create. One intriguing possibility is to pair case CYOA study development with artificial intelligence (AI), which could automate the creation of complex case scenarios and map interactions in real-time. AI could also be used with natural language processing to evaluate open-ended responses to CYOA prompts and route users to the appropriate scenario outcome. Such an AI-enhanced CYOA environment would offer a more realistic simulation of clinical practice, requiring trainees to formulate their own responses to open-ended prompts. AI is already being used in medical education to create virtual patients for diagnostic skills practice (see Dartmouth AI Patient Actor App [41]), generate exam-style questions [42], and serve as a tutor for problem-based learning [43]. Leveraging AI to develop CYOA-style cases could streamline the creation process and provide users with immediate feedback on their clinical reasoning. This integration of AI would ease the entry point for DBT and CYOA implementation while enhancing the quality and scope of data generated from these assessments. As medical education continues to embrace digital and AI-driven tools, the potential for CYOA and DBT assessments to transform clinical reasoning training is immense.



Comments (0)