Intestinal intussusception around a jejunal feeding tube in pediatric patients is a rare but potentially dangerous complication due to the risk of developing mechanical ileus and intestinal ischemia. In contrast, mechanical complications, including dislocations, obstructions, and material breakage, are more prevalent issues in JFTs, which are inherently prone to complications. This factor also exerts a significant influence on the long-term outcome of the procedure [4]. To our knowledge, this is the largest retrospective two-center study reporting detailed diagnostic and therapeutic courses of JFT-associated intussusceptions in children.
A review of the existing literature reveals that cases of intussusception around JFTs have been documented to a lesser extent than in the present study (Table 3) [9, 10]. In accordance with the findings of this study, sonography has been demonstrated to be a reliable imaging diagnostic method [6, 11, 12]. Laboratory abnormalities were only mentioned in one of the studies referenced; this patient exhibited hyperreninemia, hyperaldosteronism, and hypokalemia because of urinary retention, as well as an increase in CRP levels over time [13].
Despite the available experiences in the literature, intestinal intussusceptions around JFTs were managed conservatively in the vast majority of our patients. In spite of the presence of abdominal symptoms and sonographic evidence of intussusception around the JFT, the absence of clinical and laboratory evidence of acute abdomen with intestinal ischemia permitted observation of the patients with close monitoring. No case of mechanical ileus with bowel ischemia, perforation, or necrosis was identified. The only surgical intervention compromised a simultaneous reduction of the intussusception in a case of concomitant acute cholecystitis and indication for cholecystectomy in a patient with prior endoscopic JFT insertion.
All other endoscopically placed JFTs showed spontaneous reduction without further interventions. The current literature describing cases of spontaneous reduction of intussusceptions around JFTs in pediatric patients does not specify the insertion techniques [1]. Therefore, this is the first report on successful conservative management of intussusceptions around JFTs in children with endoscopic insertion of a jejunal access.
In contrast, Kakiuchi et al. reported on a case of strangulated ileus requiring surgical reduction of an endoscopically inserted JFT [13]. In a systematic review, Morse et al. estimated the risk of intussusception per procedure to be 1.2%, excluding blind guidewire exchange, confirming a low but still significant risk of intussusception [6].
Our findings are also in contrast to the procedures described for adults, in whom surgical treatment of intussusceptions around JFTs is often necessary due to triggering pathologies, such as malignancies or chronic inflammatory bowel disease [14,15,16,17,18].
With regard to the diagnostic approach, in our cohort, ultrasound identified intussusception in all cases with no further need of additional imaging. However, recent reports included ultrasound, fluoroscopic contrast studies, and computer tomography [11, 13, 19]. The laboratory values exhibited no specific patterns; there were no consistent elevations in infection or lactate levels. Still, this observation is subject to the timing of the diagnosis and should be integral to the standard diagnostic process, nonetheless.
The majority of our cases presented with typical abdominal symptoms, such as pain, vomiting, and diarrhea. A limitation of our analysis is that it does not capture cases of intestinal intussusception in asymptomatic patients, which may have led to an underestimation of the true number of intussusceptions occurring around JTFs. However, reports from the literature on complications in patients with intussusceptions around JFTs mainly focus on symptomatic patients and their outcomes [6, 11, 13].
In our cohort, intussusception occurred a median of 1.16 years after initial JFT insertion. These results confirm recent reports that adverse events such as intestinal perforation can even occur a substantial time after tube insertion [20].
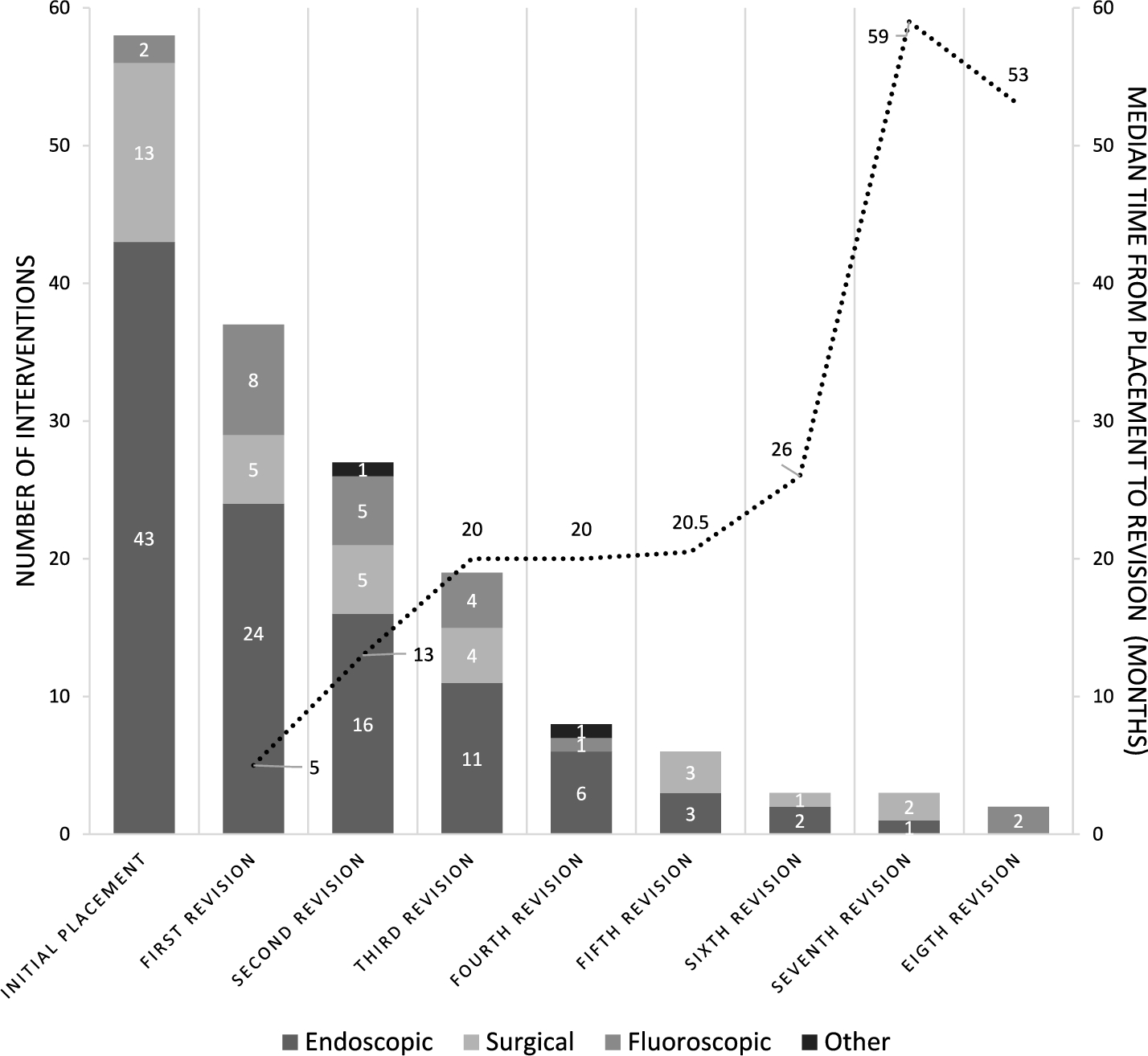
In our analysis, it however appears that the probability of intussusception increases significantly, particularly during the initial 1–2 years following initial JFT placement (Fig. 3).
As previously mentioned in the results, the cases in our cohort can be classified as minor complications according to the Clavien–Madadi classification, which incorporates non-medical errors and organizational problems into its classification of unexpected events in pediatric surgery [7, 8].
While in most institutions, the risk of intestinal intussusception around a JFT is often not recognized due to its rarity, there are various explanations and theories for the etiology. In a large cohort of 251 patients with radiologically placed JFTs, 40 intussusceptions in 30 patients were identified. The majority were treated by replacing the tube with either a standard or shortened JFT (n = 34) or a gastrostomy tube (n = 3); in two patients, an air/saline reduction was performed and the intussusception of the remaining patient was reduced surgically. Eight patients with a pigtail catheter had a recurrent intussusception, supporting the theory that the distal pigtail may catch the mucosa leading to intussusception. However, the authors also describe recurrent intussusception in pediatric patients with shortened and straight tubes. Thus, the type of tube is not considered to be the leading cause [12]. Also, in our heterogeneous cohort, no differences were observed since all of the JFTs were 9 French intestinal tubes.
Regarding the underlying diseases, it is speculated that muscle hypotonia as well as the size of the tube in relation to the bowel may be an additional risk factor [11]. In our cohort, one patient had a H3F3B mutation, which also results in reduced muscle tonus.
Another theory is that the feeding tubes cause chronic inflammation and the hypertrophied mucosa creates a lead point. This is conceivable but remains a theoretical approach without histological examination [21].
It is also important to consider that the surgical placement of the JFT usually involves the fixation of the jejunal loop to the abdominal wall. This action can serve as a pivot point for other intestinal loops, thereby promoting intussusception. This hypothesis is supported by the higher rate of volvulus observed in patients with surgically placed jejunal tubes. It was also demonstrated that major complications like an intussusception around a JFT were more frequently observed in REYJ. It is imperative that future research considers the surgical technique as a potential risk factor. Another possible risk factor for the development of intussusception is the number of revisions. Patients with intussusception underwent, on average, 2.7 revisions (no statistical testing was performed due to small sample size; data are presented descriptively) during the observation period, which is more than the average for the rest of our collective. Therefore, it can be posited that greater emphasis should be placed on the care and handling of the tube during insertion and maintenance to minimize unnecessary manipulation of the probe.
Another discussed theory (grouped under functional hypotheses) for the manifestation of the intussusception is the injecting force from the pump during feeding. It is postulated that it can drag the bowel, causing intussusception. As the majority of patients presented to our clinic in an emergency and due to the retrospective study design, this aspect could not be considered in our work. Nevertheless, this should be incorporated into prospective studies.
The available literature as well as our results illustrates the different courses of intussusceptions around JFT. As recommended by the ESPGHAN, there are different ways of inserting a jejunal tube. In our opinion, the approach should be tailored for each patient and primarily be done according to the expertise of the individual practitioner, with surgery generally being a more invasive process.
The study’s limitations can be attributed to its retrospective design and the small number of cases. Nevertheless, the present study represents one of the largest and most detailed collections of cases published to date, to our knowledge. In addition, the combination of the different types of placements by the various specialist departments (pediatric surgery, pediatric gastroenterology, adult gastroenterology, pediatric radiology) with the study design resulted in a highly varied documentation of the procedures, which led to a subsequent increase in the potential for error. Also, the potential for different treatment approaches cannot be excluded due to the interdisciplinary care provided; spontaneous reduction might also have occurred in the cases of interventional treatment for intussusceptions. Furthermore, asymptomatic transient intussusceptions could not be evaluated and may therefore have resulted in an underestimation of the true incidence.



Comments (0)