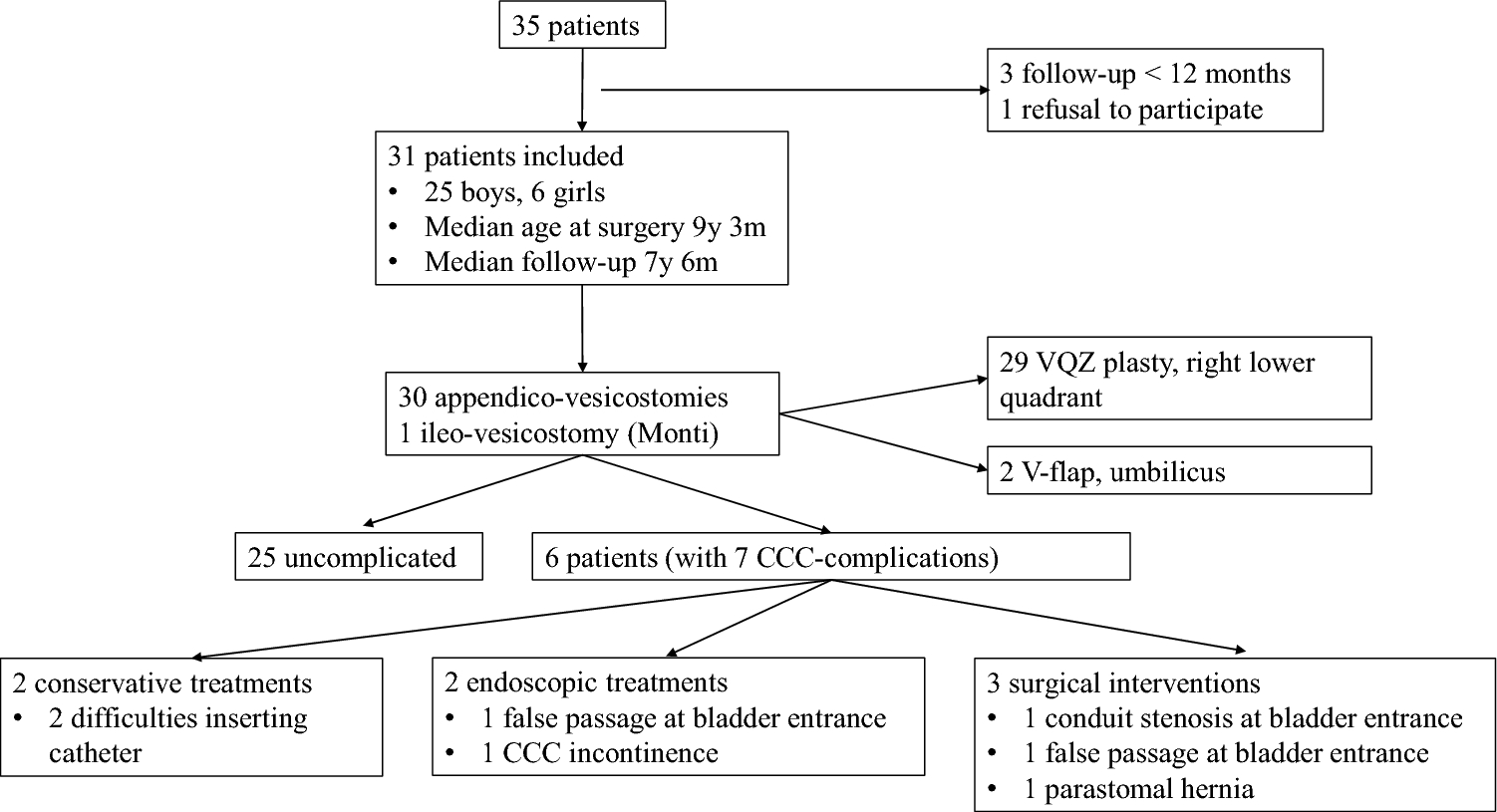
This study reports on complications after CCC surgery in our patients, mainly operated with the appendix as a conduit and a VQZ plasty at skin level. The time of their occurrence and need for surgical or endoscopic revisions were evaluated. Of our 31 patients, 6 presented with CCC dysfunction, of which 4 needed surgical/endoscopic revision. These findings reveal a notably low complication rate compared to the existing literature. This strongly suggests the efficacy of our surgical and nursing protocols.
Of note, our pediatric patient population is comparable to previously published data regarding patient age, underlying conditions, and surgical indications [[1, 2, 17, 22]. Further, our median FU of 7.5 years provides data comparable to other publications [[3, 11, 14, 16, 18, 20, 23].
General considerations
The appendix offers several advantages, being a tubular structure, severed only at one communicating end, with almost independent blood supply [[25]. As stated above, we used the appendix whenever it was available and feasible; consequently, all but one patient underwent an appendicovesicostomy. Indeed, if the appendix is unsuitable or absent, Young and Monti described small intestine use as a possible substitute [26]. It requires, however, the bowel to be detubularized in order to fashion an adequately sized channel. This structure is therefore at increased risk of ischemia and stenosis. Also, the elasticity of the bowel wall unfortunately allows for pouch formation [[4, 24]. The use of the ureter, the Fallopian tube, and conduits created of bladder or stomach wall have also been described [[6].
Depending on the publishing team, different combinations are possible between appendix versus Monti and positioning in the right lower quadrant or in the umbilicus, making it difficult to compare our series to others. Of note, all the studies report a lower rate of complications when comparing appendix to segmental ileum use. Lefèvre et al. found Mitrofanoff complications in 45% of the patients in whom they used the appendix, versus 100% of Monti channels [[14]. Faure et al. had similar findings with all Monti, ureter, and colonic conduits presenting complications compared to 61% of appendix conduits [[13]. The appendix offers a suitable diameter for catheterization, with a relatively thick wall that directs the catheter well, and a distribution of vascularization along its entire length.
In our patient population, all but two CCC were placed in the right lower abdominal quadrant. While this position leaves the stoma more visible, conduit-skin anastomosis is made of scar-free tissue and can be as wide as deemed necessary, compared to a stoma positioned in the umbilicus. Physical considerations support right lower quadrant positioning: urine drainage will be performed in a position that allows for better spontaneous outflow of urine, as well as bladder irrigation in case of entero-cystoplasty. In contrast, drainage through the umbilicus requires an upward flow, potentially leading to incomplete emptying of the bladder and hindering mucus clearing, with increased risk of infection and bladder stone formation. Opinions on stoma positioning differ. Lefevre et al. found more complications in right lower quadrant stoma positioning (54%) vs umbilical positioning (25%), perhaps because a VQZ plasty is only used in 69% of right lower quadrant stomas [[14]. Leslie finds no difference in complications between a right lower quadrant stoma and an umbilical stoma [20]. For Faure, stenosis occurs more frequently in umbilical CCCs [13]. Overall, the choice of stoma positioning remains an issue of preferred style whereas VQZ plasty has been widely adopted. While the many differences in creating the CCC as well as positioning and fashioning the cutaneous stoma speak to the fact that not one single technique is clearly superior, the long-term course of our patients compared to other experiences supports our approach (Table 5).
Table 5 Data from literature review regarding continent catheterizable channels (CCC)Types of complications
As mentioned above, compared to the literature our CCC complication of 20% was rather low. Table 5 summarizes the recent literature in the field. When analyzing CCC using mainly the appendix as a conduit, the general complication rates vary between 12 and 63% [3, 9, 13, 14, 16, 18, 20]. According to the literature, most complications consist of catheterization difficulties or conduit incontinence. With regard to catheterization difficulties, publications detail superficial (cutaneous/supra-facial) or deep (sub-facial) stomal stenoses, including angulations, strictures, and false tracts.
Superficial stenoses: To create the stoma at the cutaneous level, direct suturing is the most straightforward approach [9]. Yet, to establish an easily accessible channel, spatulation of the conduit and creation of a V-flap sutured in the conduit is possible. This is believed to reduce the rate of cutaneous stomal stenosis. However, this technique has been linked to issues in relation to the exposed mucosa such as bleeding, mucus secretion, and a less than desirable cosmetic outcome [6, 10]. To overcome these drawbacks, the VQZ-plasty, first introduced by Ransley, adopts the advantages of the V-flap and covers the intestinal-cutaneous anastomosis with a skin flap, hereby concealing the stoma and protecting the mucosa [[10]. Reported rates of superficial stenoses vary between 6 and 31% [9, 13, 14, 16, 20]. None was observed in our study. Possible explanations might be in our surgical technique with wide conduit-to-skin anastomosis, a generous VQZ-plasty, and a protocol to keep an indwelling catheter for four weeks postoperatively, avoiding repetitive manipulation of the initially vulnerable tissue.
Subfacial stenoses: they are reported to occur at a rate of 2 to 13% [9, 13, 14, 16, 20]; in our study, we observed 10%, which situates us in good company.
CCC incontinence: this complication has been reported to occur at rates of 2–10% [3, 16, 18, 20], but can reach 17% or even 24% of patients, depending on the series [13, 14]. In our series we report a low rate of 3%, treated endoscopically. In the long-term survey results, none of the 21 patients reported this complication.
CCC prolapsus: they have been described in 1 to 6% of patients [9, 13, 16, 18, 20]. Again, in our study no patient was observed with this complication.
Timing of complications
Secondary procedures were needed at 1, 12, and 20 months, then later at 4 and 6 years after the initial CCC surgery. It seems that the majority of CCC complications occur within the first two years after surgery. However, complications also may occur in the late postoperative period, with conservative management still being possible. These results are consistent with published data, reporting channel complications requiring surgical revision within 24 months [9, 18, 27]. Yet, Leslie et al. described a 30% stenosis rate in the first 3 postoperative years [20], and Szymanski mentioned the first 5 postoperative years as at increased risk for subfascial stenosis [16]. Indeed, complications are now increasingly described as occurring at any time, including in the long term, as the follow-up period increases. Jacobson et al. published in 2017 results that differ from their first analysis in 2006 with a shorter 28-month follow-up [28].
Management of complications
Of the seven CCC dysfunctions, two cases of catheterization difficulties were managed conservatively. In both cases, mucosal edema played a significant role, resolving within 1 to 4 weeks of continuous drainage with an indwelling catheter. Two patients could be treated endoscopically. Only three patients, i.e., 10% of all patients, needed surgical revision, clearly below the reported rates, ranging from 38 to 61% [13, 14, 20]. Only Welk et al. have a similar 13% revision rate [9] and Kroll et al. with a 5% rate [3].
This said, as for the different management methods, some authors detail a “minimally invasive” management combining conservative ± endoscopic treatment, while others make subgroups between superficial surgery (supra-facial) and cystoscopy versus deep surgery (sub-facial). Thus, Faure et al. reported a conservative and endoscopic management rate of 82% [13], Welk et al. 44% [9], while in our series this rate is 57%. Complications have been reported to be managed surgically (open or endoscopic) in 60% of cases by Jacobson et al. [18] (including, however, Malone redo surgeries), 78% for Welk et al.[9], 77% for Lefèvre et al. [14] and 71% for our series.
Short- and long-term surveillance
Our results show that our current surgical and nursing protocol results in very satisfying results. This said, we believe that the low complication rate observed during the FU period in our study can be attributed not only to the surgical techniques involving the appendix as a conduit and the VQZ plasty in the lower right abdomen, but also, undeniably, to the comprehensive nursing care provided. The constant and long-standing availability of our nursing staff, the ease with which patients can communicate with them regarding CIC difficulties, and their close involvement are critical factors that significantly contribute to the favorable outcomes reported. Not only do they provide practical hands-on instructions and tips on CIC, but the presence of this dedicated team also increases adherence of young people to their daily care and motivation of parents to support their child [29, 30]. Educational nurses also create a support system for the families, especially involving school nurses, to help them reach individualized goals step by step, to adapt to rhythms of family life, and to solve problems in day-to-day life. This team creates close links with patients, decreasing anxiety prior to the surgery, and following them during adolescence, supporting the transition from parental to child responsibility [31,32,33,34]. Indeed, in recent years specialized programs for children with complex medical conditions have emerged, and several studies published over the last decade report their significant positive impact on the care of both children and families [35, 36]. These programs not only improve long-term compliance but also reduce the use of emergency services and unplanned hospital admissions.
The value of long-term support, both medical and nursing, is reflected in the results of our follow-up questionnaire. The first significant result was the very high response rate of 91%, providing us with proof of good long-term compliance and adherence to treatment plans. In line with the literature [18, 20], all but one patient reported daily use of their CCC. With three to seven daily catheterizations via the CCC channel and a median FU of 7.5 years after stomal creation, catheterizations add up to 7800 to 18,650 tube passages per patient at the time of this study, in some patients considerably more. This calculation shows the extreme durability that is required in any CCC and, according to our results, durability seemingly met by the appendix, arguing again for its use.
Limitations of this study reside mainly in its retrospective nature. However, patients were followed up by the same nursing and surgical team throughout the study period, allowing for a very limited amount of missing data. Furthermore, the counterbalancing strength of this study lies in the consistency of the medical team, which remained unchanged throughout the duration of the research. This continuity ensured that both surgical procedures and postoperative management were standardized, providing a robust foundation for the reliability of our findings. Since a single operative technique was consistently applied, no internal control group was available. Therefore, we compared our findings with published experiences in similar patient populations.



Comments (0)