
Remember me


This prospective crossover study was conducted at the Community Revitalization Center, Kobe University Hospital. The performance, accuracy, and stress responses of pediatric surgeons without formal training and with minimal experience in robotic surgery were compared using the hinotori™ Surgical Robot System (Medicaroid Inc., Kobe, Japan) and conventional laparoscopy under simulated pediatric conditions.
Surgical platforms and simulated environmentThe hinotori™ system comprises a master console and three robotic arms equipped with a 10-mm, 30° videoscope and two 8-mm ports. Laparoscopic tasks were performed using conventional 5-mm instruments and trocars. All procedures were performed using the Endowork Pro II (Kyoto Kagaku Co., Ltd., Kyoto, Japan), a transparent acrylic training box with an internal volume of approximately 1,400 mL. This configuration was selected based on a previous study, which demonstrated that this volume simulates the abdominal cavity of a 6-month-old infant (weighing approximately 8 kg) [11]. Each surgeon performed robotic and laparoscopic tasks, with the order of approaches randomized to minimize potential learning bias.
ParticipantsTen board-certified pediatric surgeons participated in the study. All participants had at least 5 years of surgical experience but no formal robotic training, and most had minimal-to-no prior exposure to surgical robots. The baseline demographics of the participants are presented in Table 1. Written informed consent was obtained from all participants before the study. The protocol was approved by the Institutional Review Board of Kobe University Hospital (IRB No. B250031).
Table 1 Baseline demographics of participantsSurgical tasksTwo standardized tasks were performed using both modalities:
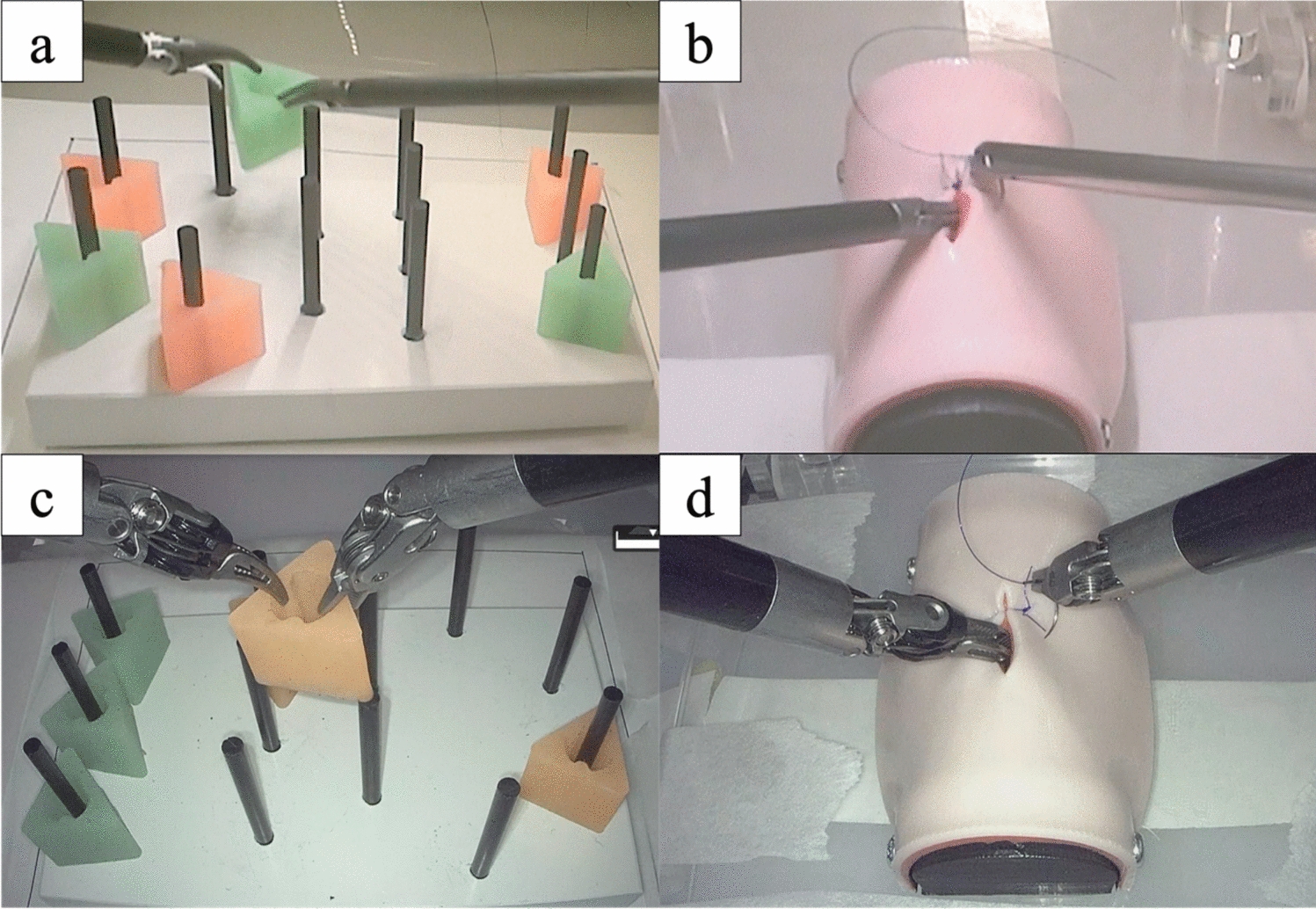
Task 1: Peg transfer (Fig. 1a–c):
Fig. 1
Experimental setup and procedural tasks. a Peg-transfer task using conventional laparoscopy. b Peg-transfer task using the hinotori™ Surgical Robot System. c Intracorporeal suturing task using laparoscopy. d Intracorporeal suturing task using the hinotori™ system
Adapted from the Fundamentals of Laparoscopic Surgery (FLS) curriculum, this task required participants to transfer six triangular blocks from one side of a 12-peg board to the other and back using Maryland graspers. Each round trip constituted one set, and three sets were completed per trial. A 1-min practice session was allowed before the task.
The FLS score was calculated using the following formula [12,13,14]:
$$300 - \left( }\,}\,}} \right) - \left( }\,}\,}\,}\,}\,}} \right).$$
Task 2: Intracorporeal suturing (Fig. 1b–d):
The participants performed three single-knot sutures on a four-layer artificial intestinal model (A-Lap Mini, Kyoto Kagaku Co., Ltd., Japan) using 8-cm-long 5–0 polydioxanone sutures with closed-eye flat needles (Ethicon, Johnson & Johnson, Germany) [15,16,17]. Each suturing was limited to 5 min, and no prior practice was allowed. All sessions were video-recorded and blindly assessed by an independent pediatric surgeon.
Outcome measuresPerformance metricsFor peg transfer, the FLS scores and number of internal instrument collisions were recorded. For the suturing task, accuracy was assessed using the A-Lap Mini system (Kyoto Kagaku, Kyoto, Japan), a computer-assisted device that automatically quantifies suturing performance. The system provides objective scores across five components:
1.Performance time: total time required to complete three stitches
2.Air leak pressure: intraluminal pressure at which leakage occurs following anastomosis.
3.Suture tension: tensile force applied to the suture during knot tying
4.Number of full-thickness sutures: number of stitches penetrating all four layers of the intestinal model
5.Wound opening area: area of dehiscence observed under pressurization, with smaller openings indicating greater suturing precision
The validity and reproducibility of these automated measurements have been demonstrated in previous studies [15, 16].
Each component was rated on a scale of 0–5, yielding a maximum total score of 25. Performance feedback was not provided between tasks.
Stress and fatigue assessmentsPhysiological stress was evaluated using heart rate (HR) and salivary amylase activity (SAA), measured pre- and post-task using a fingertip pulse oximeter and portable monitor (Nipro Corp., Osaka, Japan), respectively [18,19,20,21]. Subjective fatigue was assessed using the Chalder Fatigue Scale (CFS) and the Visual Analog Scale (VAS) for fatigue [22,23,24]. Differences (Δ) between pre- and post-task values were calculated for each parameter.
Statistical analysesStatistical analyses were performed using JMP Pro version 18 (SAS Institute Inc., Cary, NC, USA) [25]. Median values of paired comparisons (robotic vs. laparoscopic) were analyzed using the Wilcoxon signed-rank test. A p value of < 0.05 was considered statistically significant. Exploratory analyses were carried out to examine the associations between task performance and stress/fatigue indices. Pearson’s correlation coefficients (r) with 95% confidence intervals were calculated, and robustness was assessed using Spearman’s rank correlation (ρ) as SAA values exhibited skewness and potential outliers. To further assess sensitivity, SAA values were winsorized according to the interquartile range (IQR), and the analyses were repeated. As these analyses were exploring, no adjustments for multiple comparisons were applied.
Comments (0)