In the overall population of our study, patients who underwent SG showed significantly better survival than those who underwent WR. However, the effect of WR and SG on survival in patients with part-solid tumors was significantly different from that in patients with solid tumors. Solid-type tumors were independently associated with a worse prognosis.
Among patients with solid-type tumors, recurrence was more frequently found in patients who underwent WR than in those who underwent SG; however, this was not observed in patients with part-solid tumors. Part-solid tumors were associated with significantly better survival and less invasiveness (i.e., low c-stage, dominant adenocarcinoma, and negative pleural and lymphovascular invasion) than solid tumors, which may be related to their superior clinical background (e.g., lower frequency of smoking history). Thus, based on the current data, it can be said that WR was inferior to SG in the overall population and in patients with solid-type tumors, but it was equivalent to SG in patients with part-solid-type tumors with a relatively low malignant status.
In comparison with WR, anatomical SG has the theoretical advantage of achieving appropriate margins and wider resection of the draining lymphatics, including intersegmental planes commonly referenced as a source of residual cancer cells [6, 7]. However, several studies that compared WR and SG have reported different outcomes. Altorki et al. described SG and WR as equivalent for peripheral NSCLC < 2 cm in size in a post hoc analysis of CALGB140503 [8] and another retrospective study [9]. In an STS database analysis, WR showed comparable outcomes to SG in patients with c-stage IA disease [10]. In contrast, several meta-analyses have suggested that WR is inferior to SG [11, 12] in stage IA disease. A recent report from the Japanese Joint Committee of Lung Cancer Registry (JJCLCR) database showed that SG was equivalent to WR in patients with cT1a disease, whereas SG was significantly superior to WR in cT1b [13]. A retrospective study by Koike et al. also reported that SG significantly improved survival relative to WR in patients with c-stage IA disease [14].
Preoperative HRCT findings of CTR provide great insight into tumor aggressiveness [15, 16]. Hattori et al. reported that adenocarcinoma cases with a CTR of < 1.0 often had a lepidic component and showed a good prognosis and less invasiveness, even if the accompanying GGO was small [17]. This finding is consistent with the results of our study. According to their results, LN metastasis and lymphovascular invasion were rarely found in cases with CTR < 1.0, which suggests that SG, which allows lymphatic dissection [6], might not be necessary for tumors with CTR < 1.0, as long as a sufficient margin can be obtained. However, CTR = 1.0 sometimes causes LN metastasis because patients often have pleural invasion, lymphatic and vessel invasion, and high-grade malignant subtypes [17]. This indicates that WR often causes locoregional recurrence and that SG might be preferable in cases with a CTR of 1.0.
WR is typically performed in high-risk patients. The criteria used to determine whether WR or SG should be performed have not yet been clarified. SG is a superior oncological approach to WR; however, it is more invasive. In the current study, severe postoperative complications (Clavien–Dindo classification ≥ III) were more frequently found in SG than in WR (6.2% vs. 2.4%, p = 0.19), especially for pulmonary complications (5.2% vs. 1.6%, p = 0.25), despite the worse background of the WR population, although the difference was not significant. In fact, SG was slightly inferior to WR for part-solid tumors in terms of OS (94% vs. 98%), although the difference was not significant. The JCOG 0804 trial showed that WR offers sufficient outcomes for peripheral GGO-dominant tumors if a surgical margin is obtained [3]. Generally, SG requires a larger lung parenchyma resection and longer operation time; therefore, invasiveness and curability should be balanced. A Japanese prospective trial (JCOG1909) to determine the superiority of anatomical segmentectomy over wedge resection in high-risk operable patients with clinical stage IA NSCLC is currently ongoing. Therefore, the results should be carefully reviewed [18].
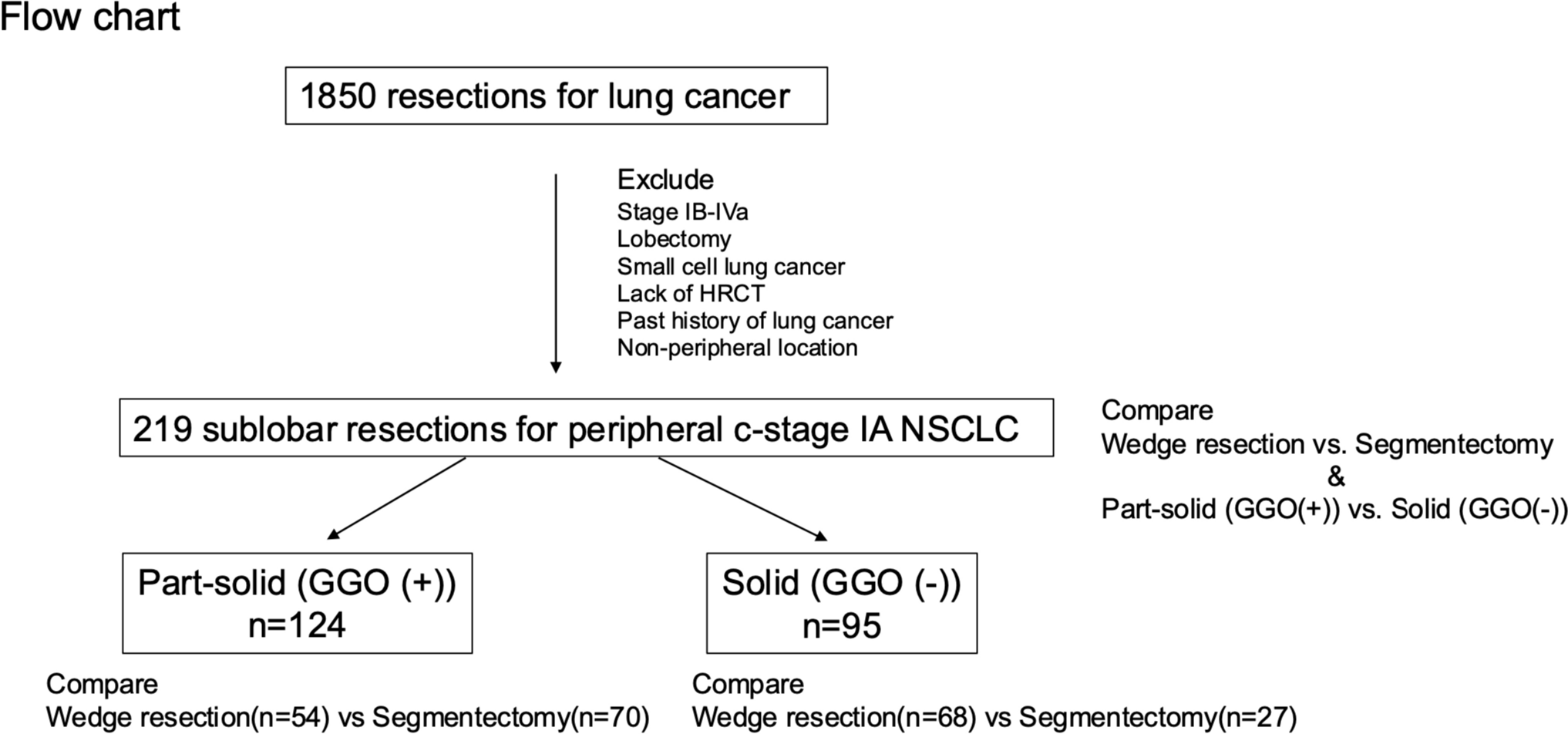
Our data showed that part-solid (GGO (+)) was an independent good prognostic factor and was well controlled by WR. The CTR is a simple surrogate marker that can be assessed using HRCT alone. Previous Japanese studies classified the CTR in detail (e.g., 0.25 and 0.5) and demonstrated its utility in predicting malignancy [15, 19]; however, it is considered less objective because it is evaluated by only 2-dimensional imaging and there may be overlapping cases (e.g., one evaluator determines that the CTR of a tumor is 0.51, while others determine that it is 0.45). Classification using part-solid (GGO (+)) or solid (GGO (−)) seems to be a simple and reliable method for predicting malignancy and determining the surgical procedure without PET/CT, which is not available in some hospitals. However, the solid type (GGO (−)) contains several pathological subtypes that differ in terms of malignancy. Accordingly, this population requires further studies using other biomarkers or modalities (e.g., PET-CT) to predict tumor invasiveness [20,21,22].
The present study has several limitations. First, this was a retrospective study, and the selection of patients for either WR or SG was not random. Most sublobar resections in this study were performed because of the high-risk background. The baseline characteristics differed between the WR and SG groups. To reduce this bias, a propensity score-matched analysis was performed after matching for comorbidities. Furthermore, we used LCSS, DFS, and OS, which are closely related to recurrence rates and control for the impact of other causes of death. For the solid type, DFS and recurrence rates were significantly different between WR and SG, whereas differences in LCSS and OS were not statistically significant between WR and SG, even though propensity score-matched analysis was performed. This means that both cancer recurrence and other causes of death were more frequent in the WR group than in the SG group. In fact, it is difficult to verify the intensive indication for limited resection (especially for WR), which was not standard at that time. Therefore, we used real data for the passive indications. Prospective randomized controlled trials are needed to validate these intensive indications. Second, we did not have information on resection margins. Previous studies have shown that a narrow surgical margin (i.e., ≤ 1 cm) is associated with local recurrence [23, 24]. In the current study, locoregional recurrence after SG was favorable (4.1%), which might reflect a relatively wide surgical margin in comparison to WR. Moreover, intraoperative lymph node evaluation by frozen-section examination is rarely performed, especially in cases with a high risk of conversion to lobectomy, because conversion of the surgical procedure to lobectomy is difficult if positive nodes are identified intraoperatively, and shortening of the operation time is considered important. Finally, tumors were not stratified by CTR because the sample size was small, and surgical procedures were determined by patient condition rather than tumor condition in this study. CTR stratification is also important for determining the oncologically optimal surgical procedure (e.g., GGO-dominant T1a tumor should be distinguished from a solid-dominant part-solid T1c tumor). Despite the above limitations, the surgical outcomes after WR and SG in our study were not inferior to those of the previous randomized controlled study [1, 8].
In summary, among patients with c-stage IA peripheral NSCLC who underwent sublobar resection, part-solid cases showed a better prognosis than solid cases. SG was superior to WR for peripheral c-stage IA NSCLC, although WR was equivalent to SG for part-solid-type tumors.



Comments (0)