In this retrospective single-center study, we demonstrated that patients with extensive CAD, identified using the CT-BCIS-JS, have an increased risk of mortality and rates of MACE as compared to patients with non-extensive CAD. To our knowledge, this is the first study to assess the prognostic value of the CT-based BCIS-JS, emphasizing its utility as a clinical tool not only for the assessment of the extent of jeopardized myocardium pertinent to obstructive CAD, but also for risk stratification.
This study approached extensive CAD as an important clinical indicator that should be easily and reliably recognized by non-invasive imaging. The clinical significance of extensive CAD, identified using invasive coronary angiography but also employing CCTA, has been previously described in several studies [5, 9, 24]. In a retrospective analysis of the Prospective Multicenter Imaging Study for Evaluation of Chest Pain (PROMISE) trial, high-risk CAD, defined as left main stenosis ≥ 50% stenosis or ≥ 70% stenosis of 3-vessels or 2-vessel CAD involving the proximal left anterior descending artery, was associated with more frequent invasive interventions and adverse events [5]. In a more recent sub-analysis of the International Study of Comparative Health Effectiveness with Medical and Invasive Approaches (ISCHEMIA) trial, although patients with left main disease were excluded, the authors also showed a graded association between CAD severity and adverse cardiovascular events [24]. Our results build on and extend these findings by demonstrating, in an observational setting, the prognostic value of a global metric that quantifies the extent of jeopardized myocardium.
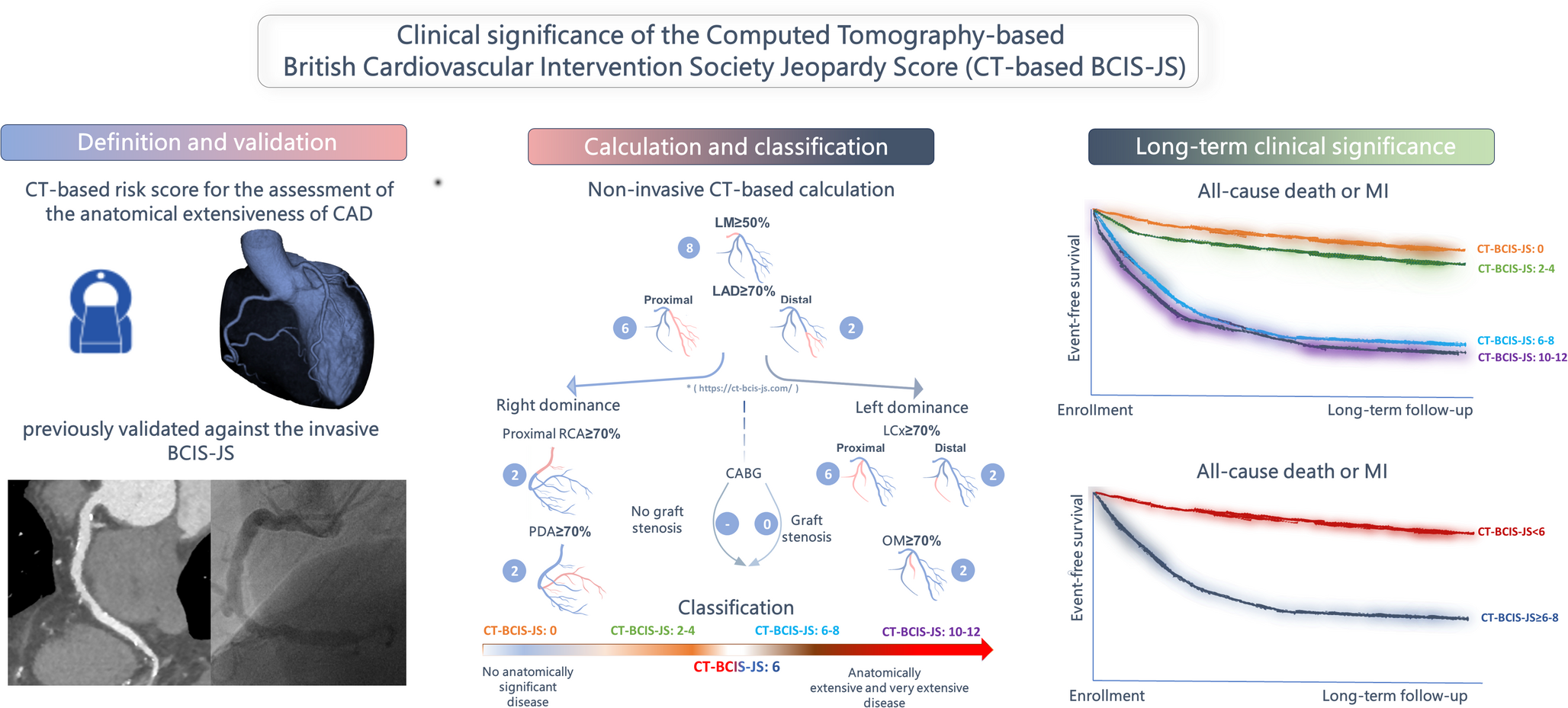
The invasive BCIS-JS, long proposed as a simplified angiographic scoring system for identifying patients with extensive CAD, has limited data supporting its prognostic significance [17]. Its ability to predict mortality was retrospectively demonstrated using the ‘Revascularization Index’, which compares pre- and post-PCI BCIS-JS scores [14]. The completeness of revascularization using the jeopardy score was an independent predictor of all-cause mortality, and the pre-PCI BCIS-JS score was directly related to mortality [14]. The respective CT-based score has been recently validated, showing excellent correlation and agreement with its invasive counterpart, along with very high reproducibility [15]. Several other CT-based CAD scoring systems, such as the CT-based modified Duke Prognostic Index, the Segment Stenosis Score (SSS) and the Segment Involvement Score (SIS), have proven effective in distinguishing complex CAD and predicting outcomes. However, each system has its own limitations, and few have been validated against their invasive reference standard [8, 10]. The BCIS-JS provides a distinct approach to risk stratification compared to established CT-based scores. While SIS and SSS reflect the overall burden and severity of coronary atherosclerosis by counting involved segments or weighing stenosis severity, they do not incorporate information on the amount of myocardium at risk. The extensively studied SYNTAX scores I and II are comprehensive angiographic grading tools that incorporate anatomical and clinical factors to assess CAD complexity [11, 25]. Although the invasive SYNTAX scores have prognostic implications, the CT-based SYNTAX scores are primarily used in revascularization decision-making, but their calculation is complex and time-consuming [13, 26]. In contrast, the CT-derived BCIS-JS estimates the extent of jeopardized myocardium based on the presence of high-grade stenoses in major coronary territories, thereby linking anatomical disease with potential functional impact. This may enhance its clinical relevance, particularly in identifying patients more likely to benefit from revascularization. In our study, CT-based BCIS-JS was significantly associated with long-term cardiovascular events, supporting its value as a practical, functionally oriented risk stratification tool following abnormal CCTA. While we did not directly compare BCIS-JS with other CT-based scoring systems, its conceptual focus on myocardial jeopardy offers complementary prognostic insight beyond anatomical burden alone.
In contrast to Coronary Artery Disease Reporting and Data System (CAD-RADS), which primarily focuses on the most severe stenosis and serves as a standardized framework for reporting and management guidance, the CT-BCIS-JS provides a comprehensive, semi-quantitative estimate of the total myocardium at risk. While CAD-RADS grades the lesion and includes modifiers for high-risk plaque features, stents, or grafts, it does not account for lesion distribution, coronary dominance, or graft patency, nor does it offer a summative burden of disease. The CT-BCIS-JS systematically evaluates all major coronary territories, including native vessels and bypass grafts, integrating anatomical complexity and extent of ischemic myocardium into a reproducible numeric score. The CT-BCIS-JS can complement and extend the information provided by CAD-RADS, offering a more complete assessment of coronary disease burden and aiding in revascularization planning. It is further important to note that the CT-BCIS-JS does not quantify total plaque burden, but rather estimates the extent of myocardium at risk based on the location and severity of obstructive lesions. In clinical practice, both total plaque burden and CT-BCIS-JS may be used in a complementary fashion, as they provide distinct yet synergistic information relevant for risk stratification, ischemia assessment, and revascularization planning.
The primary advantage of the CT-BCIS-JS lies in its ability to quickly and easily provide reliable estimates of CAD extensiveness using an online calculator. This system is particularly valuable for assessing patients with left main lesions and bypass grafts, which are often omitted in other angiographic scores. A CT-BCIS-JS score of ≥ 6, corresponding to approximately 50% of the left ventricular myocardium at risk, was used as an inclusion criterion in the REVIVED-BCIS2 trial [21]. Although the trial did not formally validate this threshold, its use highlights the clinical relevance of the ≥ 6 cutoff for identifying patients with substantial myocardial jeopardy. Our findings support the prognostic value of this threshold; patients with CT-BCIS-JS scores ≥ 6 experienced significantly more events and worse outcomes, while those with scores of 0 and 2–4 had similarly low event rates. This non-linear pattern likely reflects the categorical structure of the score, which was designed to distinguish between non-extensive and extensive CAD rather than to provide a continuous gradient of risk. The limited number of score categories and small sample sizes in the intermediate groups may also have contributed to the observed clustering of outcomes. By focusing primarily on stenoses in the proximal coronary tree, devoid of complicated plaque analyses and incorporating coronary dominance, the CT-based BCIS-JS was demonstrated to hold substantial prognostic value. This makes it a potential effective tool for identifying patients with extensive CAD, improving personalised risk stratification, and informing need for subsequent testing as well as management decisions.
This study should be interpreted in the context of certain acknowledged limitations. First, despite the application of multivariable adjustments, our results remain susceptible to unrecognized biases inherent in retrospective observational studies and unmeasured confounding factors. Additionally, our study was single-centered and had a relatively limited sample size. However, the significant number of events allowed for a robust assessment of the predictive value of the CT-BCIS-JS. In addition, our cohort included patients with both known and previously undiagnosed CAD, which may have introduced heterogeneity in terms of baseline risk, clinical management, and secondary prevention strategies. Although statistical models were adjusted for history of CAD and major cardiovascular risk factors, residual confounding related to differences in care pathways cannot be entirely excluded. Moreover, this study included many patients with extensive CAD, constituting a group likely not representative of the currently lower-risk patients undergoing CCTA. Furthermore, MIs were defined based on the previous definitions, which presents some differences compared to the fourth universal definition that is currently used. Additionally, coronary calcium scoring, and detailed plaque quantification were not available, two important parameters also associated with adverse outcomes. While our study was not designed to compare CT-BCIS-JS directly against CAD-RADS or other existing scoring systems, our results underscore its independent prognostic value. Future studies are warranted to evaluate its incremental benefit over established frameworks in larger and more diverse populations.



Comments (0)