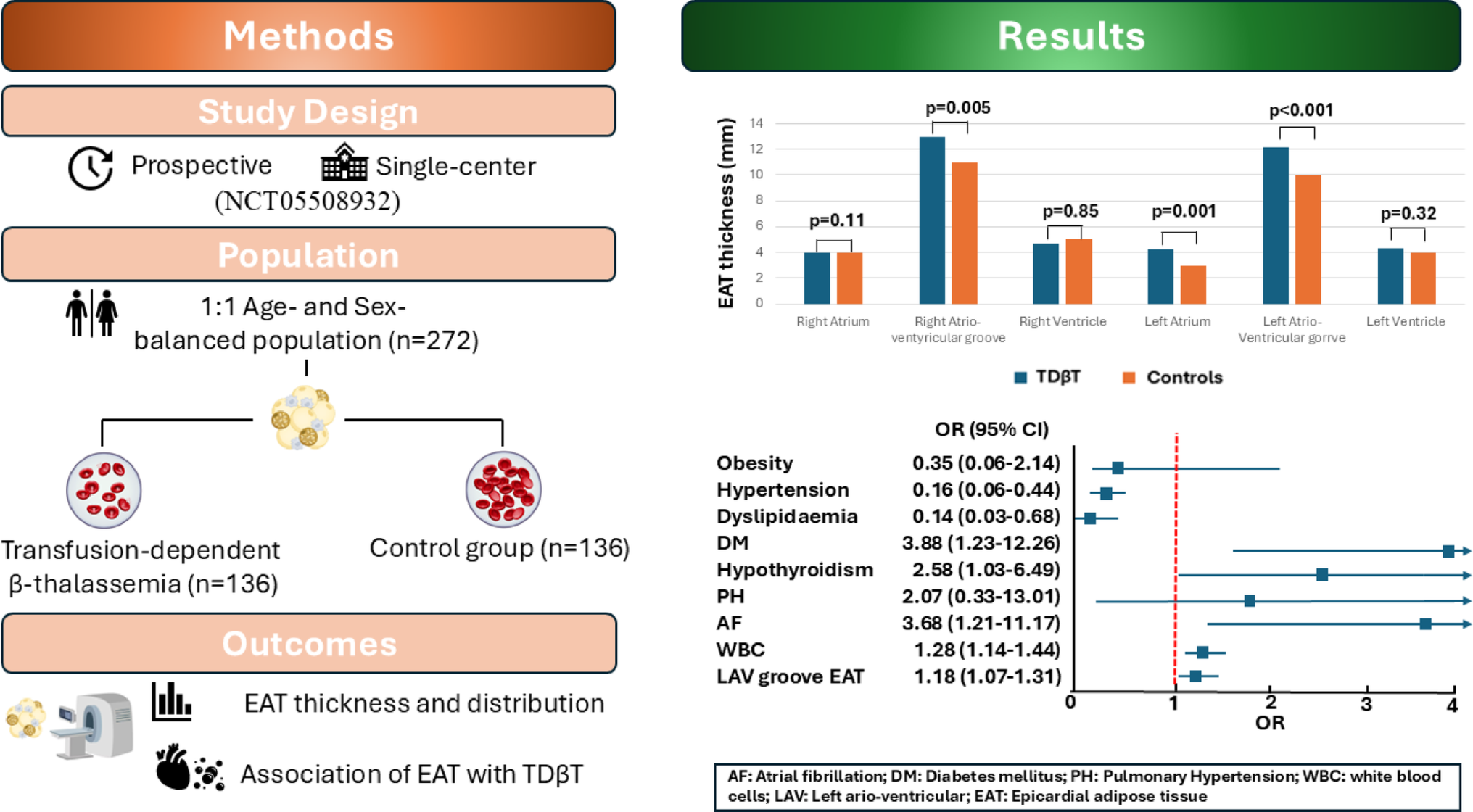
The main findings of our study are as follows:
EAT was significantly higher in patients with TDβT than in controls.
Differences were found in the regional distribution of EAT between patients with and without AF, diabetes mellitus, stroke and heart failure.
To the best of our knowledge, this is the first study comparing thalassemic patients and non-thalassemic controls focused on EAT. While the role of EAT in cardiovascular disease pathophysiology is well established, the association between EAT and TDβT is a novel finding that raises important new questions and hypotheses. Per se, patients with thalassemia are at increased risk of developing comorbidities such as AF, diabetes mellitus, stroke and heart failure, all of which share EAT as a common risk factor. Furthermore, patients with TDβT have a higher prevalence of other comorbidities, like hypothyroidism and pulmonary hypertension, for which the role of EAT has not been explored. The presence of multiple baseline differences between the study group and control group shouldn’t be surprising as this reflects the complex health conditions of patients with thalassemia [4]. In our results, the multivariate analysis confirmed the independent association between EAT and TDβT. However, understanding the pathogenetic role of EAT in this context exceeds the scope of our study, but our results represent important findings that will need further investigations.
Moreover, our results showed that AF, hypothyroidism and diabetes mellitus were independently associated with TDβT. The prevalence of AF in our study group was 27.9%. This finding aligns with recent studies among AF in thalassemia, which reported prevalence rates of 14–29% [16-19]. These rates of AF among patients with thalassemia are impressively higher than the 2–4% documented in the general population [13]. Historically, cardiac iron overload was a primary cause of arrhythmias in TDβT patients [20, 21]. However, with the advent of regular iron chelation therapy, the natural history of the disease has changed. Recent prospective studies conducted in contemporary cohorts, specifically investigating the relationship between arrhythmias and iron, found that AF was unrelated to iron overload [18, 22]. Confirming this, in our study patients with cardiac iron overload at the most recent MRI were only 3.7%. A combination of factors underlies the higher prevalence of AF in thalassemic patients, among which a role is played by anemia, inflammation, chronically elevated cardiac output, atrial fibrosis and remodeling [2]. In addition to those factors, EAT may play a role. The independent association between EAT and AF, which is well established in the general population, has been observed and confirmed in patients with TDβT in a previous observational study conducted by our research group [18]. However, a major limitation of that study was the absence of a control group to be compared with thalassemic patients. Our current work addresses that limitation and enhances our understanding of EAT role in this setting.
Hypothyroidism and diabetes mellitus are among the most common comorbidities in thalassemia, a finding also confirmed by our study population [4]. Conversely, we observed a significantly lower prevalence of arterial hypertension in patients with TDβT. In the general population, arterial hypertension is one of the most common risk factors associated with AF [23]. This observation is not unexpected, as the mechanisms underlying the development of AF in thalassemia are, at least in part, different from the general population [2, 4]. It can be hypothesized that, in the context of β-thalassemia, arterial hypertension may play a lesser role in the development of AF compared to other factors. However, further studies could provide additional understanding of those observations.
Our results showed differences in the regional distribution of EAT between patients with and without TDβT. Specifically, thalassemic patients showed higher EAT values at the left atrium and at both atrio-ventricular grooves. Previous studies have suggested that the regional distribution of EAT may influence the development of various diseases such as AF, heart failure or coronary artery disease. For example, only EAT at the left atrium was associated with AF, while pericoronary EAT was associated with coronary artery disease [8, 24]. EAT affects the adjacent myocardium through the secretion of cytokines that promote inflammation (e.g., IL-6, tumor necrosis factor) and fibrosis (e.g., activin A, tissue growth factor, matrix metalloproteinases), as well as through the infiltration of free fatty acids and autonomic disorders via ganglionated plexi. At the atria, one consequence of these effects is AF. Notably, our study found that EAT in TDβT patients was higher at both atrioventricular grooves and at the left atrium, but not at the right atrium. When considering AF, diabetes mellitus, stroke and heart failure, no differences were observed at the atrioventricular grooves. Moreover, the association between EAT at left atrioventricular groove and TDβT was independent from other variables. We could hypothesize that the higher distribution of EAT at the left and right atrioventricular grooves may be characteristic of thalassemia. Other parameters, such as the fat attenuation index assessed by cardiac CT could be useful in order to better understand two main points: the synergistic effect of EAT and inflammation on onset and chronicity of AF, the influence of thalassemia on inflammation of the pericardial fat. Further studies could provide additional insights into this finding.



Comments (0)