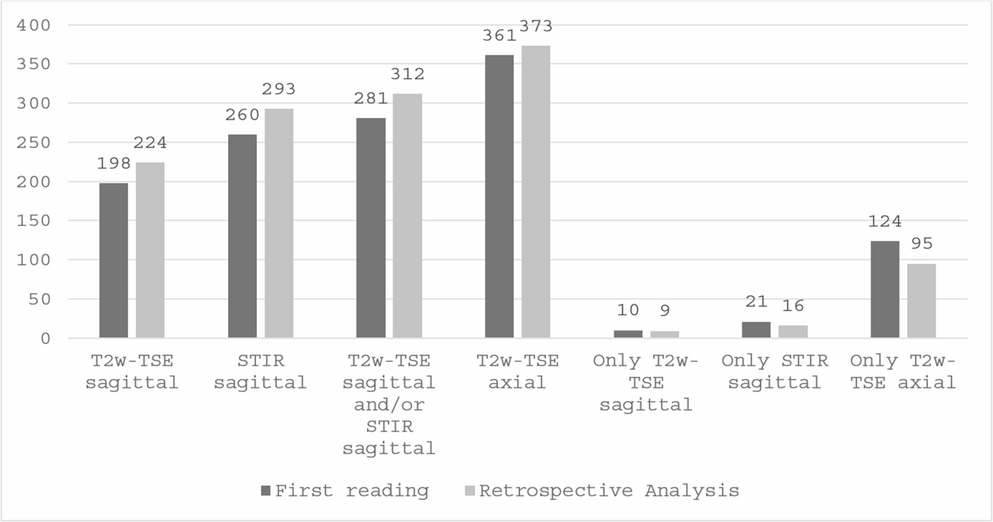
In contrast to recent recommendations [8, 9], we achieved highest detection rates for spinal cord lesions using an axial T2w-TSE sequence with full spinal cord coverage, followed by a sagittal STIR, and lastly a sagittal T2w-TSE sequence. This is not surprising, since former studies have already demonstrated the superior detection rates of axial T2w sequences with full or at least long spinal cord coverage compared to sagittal T2w sequences [10, 12]. However, these studies did not compare the detection rates of the axial acquisitions to sagittal STIR sequences. To our knowledge, this is the first study demonstrating that the axial T2w-TSE sequence detects more spinal cord lesions in MS patients than the STIR sequence, even when combined with the sagittal T2w-TSE sequence. Nevertheless, the STIR sequence does offer additional diagnostic value since it outperformed the sagittal T2w-TSE sequence in our study, which is in line with previously published results [13,14,15]. With the sagittal STIR sequence we detected 31% more lesions compared to the sagittal T2w sequence, which is similar to the results of Dietemann et al. or Nayak et al. who reported an increase of 46% and 35%. However, in the axial T2w-TSE images 67% more lesions could be detected than in the sagittal T2w-TSE images and 27% more lesions compared to the sagittal STIR sequence. Previous studies have also reported a significant increase in lesion detection using an axial T2w-TSE sequence compared to a sagittal T2w-TSE sequence, with 33.2 to 153.7% more lesions detected [10, 12]. So far to our knowledge, there are no previous studies comparing the detection rates between the sagittal STIR sequence and the axial T2w-TSE sequence.
Ninety-five lesions were only seen on axial images and could not be detected, even retrospectively, on the sagittal images. These lesions had a smaller diameter, a smaller craniocaudal extension and were more often located in the lateral spinal cord. Reasons for missing these lesions on sagittal images could be the recommended slice thickness of 3 mm of the sagittal sequences [8]. With a tapering transverse diameter of the spinal cord, which ranges in average between 13.2 mm at its widest level of C5 and 8.3 mm at T8 [16], it is possible that the spinal cord might only be fully captured in one slice and only displayed partially or with significant partial volume effects in the more lateral slices. Accordingly, more lesions were solely detected on the axial scans in the thoracic spinal cord, although this was not statistically significant.
The inter-rater agreement for all three evaluated sequences was good. However, when looking at lesions detected in the sagittal T2w-TSE images plus in an additional sequence, the inter-rater agreement was higher for the sagittal T2w-TSE sequence in combination with the axial T2w-TSE sequence compared to the STIR sequence. This is somehow surprising, since former studies have reported highest inter-rater agreement for the STIR sequence [15, 17].
We used a 3 T scanner in our study which could explain our lower inter-rater agreement for the STIR sequence. Compared to 1.5T, 3 T MRI is more susceptible to artifacts arising from B1 field inhomogeneity, susceptibility effects, and vascular pulsations, which decreases diagnostic performance especially in the thoracic spinal cord [18, 19]. Furthermore, we only excluded patients with excessive motion artifacts but still included patients with suboptimal image quality caused by movement, vascular pulsations or adiposity. In doing so, we were able to evaluate the sequences in their clinical and routine applications.
Historically, due to time consuming acquisitions of a full coverage of the spinal cord with an axial T2w sequence, it was often limited to the cervical spinal cord [20, 21]. Recent studies that investigated long or full axial coverages of the spinal cord in MS patient have shown that lesions also occur frequently in the thoracic spinal cord and are not predominantly limited to the cervical segments [10, 12]. For example, Galler et al. who used a full axial coverage of the spinal cord reported that 47.3% of all lesions found were located below C7 which is in line with our results as we detected 46.1% of all lesion within the thoracic spinal cord. With the advantage of parallel image acquisitions, the scan time for a full axial coverage of the spinal cord was 6:46 min, which is only slightly more time consuming than the STIR sequence (5:36 min). We are confident that with recently introduced imaging techniques, such as compressed sensing or deep learning-based acceleration, acquisition times can be shortened even further while maintaining or even improving image quality.
There are some limitations which we would like to address. A significant limitation of this study, consistent with previous research comparing MR imaging sequences for lesion detection in the spinal cord, was the absence of a definitive reference standard for confirming lesion presence. A lesion size of at least 3 mm has been suggested but we also included lesions with smaller diameters [2]. Without postmortem pathological data—the only truly reliable reference—we relied on the consensus evaluations of two experienced raters which is in line with previous studies [4, 10, 12, 15, 22]. However, due to the lack of a real ground truth, we refrained from determining false positive rates, limiting conclusions about diagnostic accuracy. The study sample included a broad spectrum of MS patients and those with suspected demyelinating disease, which may limit conclusions about the diagnostic value for specific MS subtypes or disease stages but also mirrors the real-world clinical population in MS day hospitals. Further, we did not evaluate the diagnostic performance of other suggested sequences for lesion detection but focused on the most commonly applied sequences for spinal MS imaging. While other sequences have also been proposed and scientifically studied, such as sagittal PDw, sagittal PSIR or axial T2w GRE, it has been shown that these sequences are still rarely used in clinical practice [23]. This is also true for 3D sequences which offer the possibility of multiplanar reconstructions. Future research should focus on optimization of sequence parameters such as slice thickness and pixel size at 3 T field strength as well as implementation of 3D sequences to improve diagnostic accuracy in lesion detection.
Our study demonstrates the superior detection rates of the axial T2w-TSE sequence with full spinal cord coverage over the sagittal T2w-TSE and STIR sequence for spinal cord lesions in MS or suspected demyelinating disease, while inter-rater agreement was comparable between the axial T2w-TSE and the STIR sequence. Including axial T2w-TSE images with full spinal cord coverage in standard imaging protocols may enhance the evaluation of disease burden and diagnostic processes in MS.

Comments (0)