Patients’ selection
This retrospective, non-interventional, multicenter study is based on patients included in the K-VIROGREF cohort (epidemiological, clinical, and immunological study of a cohort of adult patients with viral-induced cancers, after solid organ and hematopoietic stem cell transplantation). Patients with PTLD were screened from July 2013 to October 2021. Inclusion criteria were as follow: histologically proven polymorphic or monomorphic PTLD; available baseline 18F-FDG PET/CT, performed within 30 days prior treatment. Exclusion criteria were: indolent lymphomas; previously treated PTLD; Central nervous system involvement; noncompliance with fasting prior to PET; incomplete DICOM data.
The diagnosis of PTLD was made in accordance with the WHO classification [10] of malignant lymphoma and confirmed by expert hematopathologists from the Lymphopath network, according to the standard French procedures.
Data collection
For each patient, the following parameters were collected from the K-VIROGREF registry: (1) clinical data including age at diagnosis, sex, Eastern Cooperative Oncology Group Performans Status (ECOG PS), B symptoms; (2) transplantation related data: time between transplantation and diagnosis of PTLD, age at transplantation, transplanted organ; (3) lymphoma characteristics: histology, Epstein Barr Virus status of the tumor (EBER), Ann Arbor stage, Nodal involvement, extranodal involvement, graft involvement; (4) International Prognostic Index (IPI), LDH, Bêta-2 microglobulin and albumin levels; (5) Treatment strategy, including reduction of immunosuppression. PFS was calculated from diagnosis until disease progression, relapse or death from any cause or last follow-up. OS was defined from diagnosis to death or last follow-up.
Regarding 18F-FDG PET/CT: DICOM data and weight were collected.
Baseline PET measurements
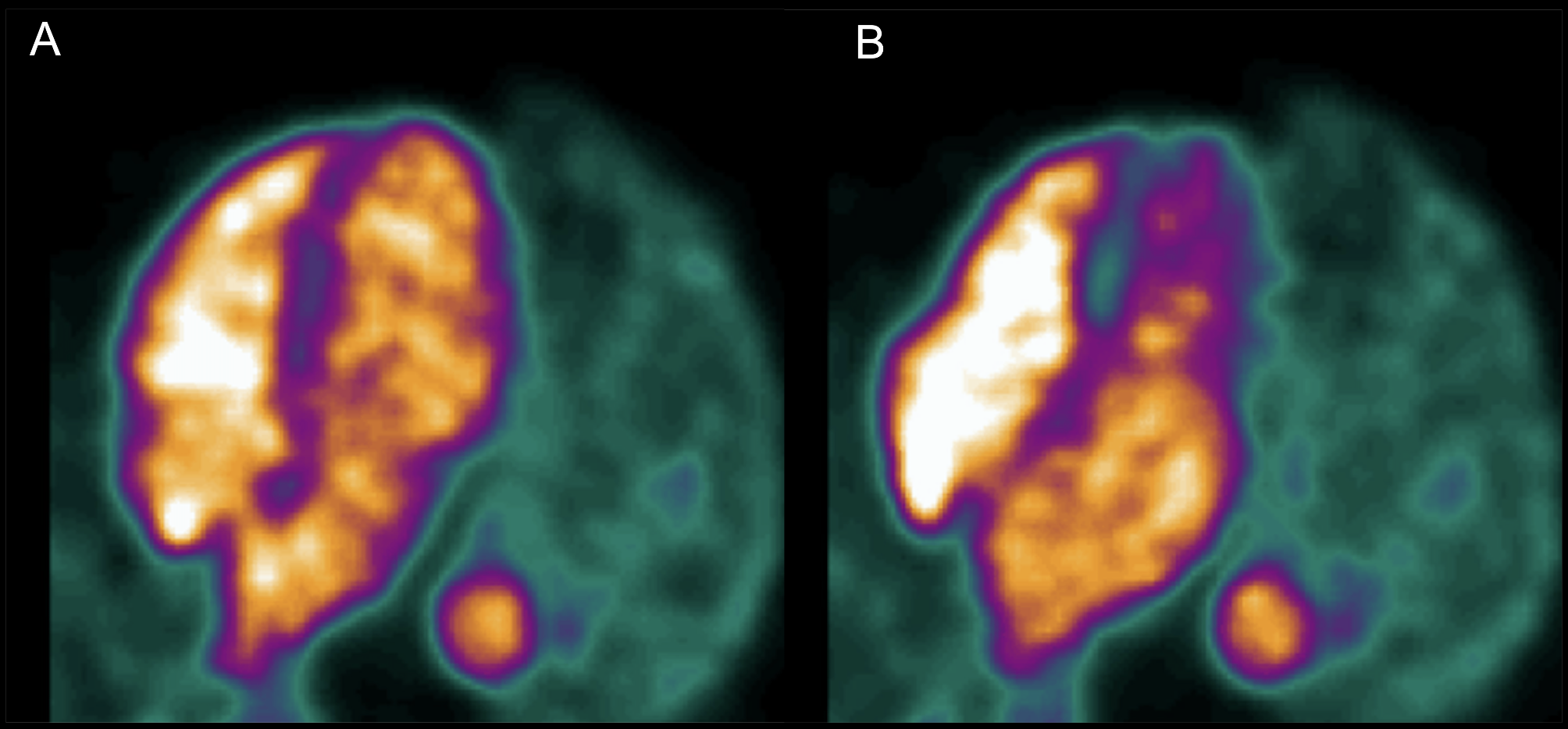
PET/CT were displayed on a dedicated interpretation console (AW server, General Electrics, USA). Cerebellum/Liver index was measured as previously described [7, 8]. The SUVmax of the cerebellum was measured using an enclosing region of interest (ROI) excluding any voxel of the neighboring brain hemispheres. A default cubic ROI of 72 cm3 (41% SUVmax threshold) was positioned in the right liver to measure its SUVmean. CLIP is the ratio of the SUVmax of the cerebellum divided by the SUVmean of the liver. This measurement technique has been proven to be reproducible and not dependent on the type of region of interest used (thresholding or not, cubic or spherical shape) [7, 8].
Total metabolic tumor volume (TMTV) and total lesion glycolysis (TLG) were obtained by summing the metabolic volumes of all nodal and extranodal lesions according to the method detailed by Meignan et al. [11] (41% SUVmax threshold, inclusion of only focal bone marrow involvement, spleen considered involved in case of focal increased uptake or diffuse increased uptake of at least 1.5 times the liver uptake).
For exploratory purposes, other parameters were measured: the SUVmax of the lymphoma lesion with the greatest uptake was collected, as was the SUVmean of the lymphoma (TLG/TMTV); SUVmean blood pool was measured using a spherical region of interest placed in the aorta. Commonly used ratios (SUVmax tumor/SUVmean liver and SUVmax tumor/SUVmean bloodpool) were calculated.
All measurements were performed by an experienced nuclear medicine physician (DM) who was blinded to the clinical data of the patients.
Statistical analysis
For descriptive analysis, qualitative variables were described by their absolute and relative frequency (%). Quantitative variables were described by mean, standard deviation. Median, interquartile range (IQR) and extreme values are provided in addition for TMTV. Comparisons between patients with CLIP < 3.24 and CLIP > = 3.24 were performed using Khi2 or Fisher exact test or Mann Whitney test as appropriate. When a significant difference was noted, spermann R2 (coefficient of determination) was performed between CLIP and the considered factor to estimate if the factors were not surrogates of one another. The threshold of 3.24 was selected ad hoc in accordance with a previous paper [8] focusing on aggressive lymphomas in immunocompetent patients.
For the main analysis: univariate and multivariate analyses using Cox models were performed. Four variable were tested at univariate analysis: IPI, TMTV, CLIP and treatment strategy (Rituximab or upfront chemotherapy). Quantitative variables were dichotomized using already published thresholds: IPI ≥ 3 [3], TMTV ≥ 220 cm3 [12], CLIP < 3.24 [8]. Multivariate analysis was conducted using a model selection approach. When several factors were collinear, only the factor resulting in the best model based on the Akaike criterion was retained. Derived hazard ratio (HR) and corresponding 95% confidence intervals (95%IC) are reported. Survival data were displayed on Kaplan Meier curves, comparisons were performed using a log-rank test. A p value < 0.05 was considered significant.
For the second objective, PET parameters including CLIP were studied both for PFS and OS using the same procedure: an optimal threshold was determined based on survival curves [13]. Relevant factors were then selected using multivariate analysis and model selection.


Comments (0)