Preoperative diagnosis of benign and malignant renal masses can guide the selection of surgical methods and prevent unnecessary nephrectomy. US be used to distinguish between benign and malignant renal masses by observing their echogenicity, shape, boundaries, capsule, blood flow, etc. Malignant masses typically exhibit hypoechoic lesion, irregular morphology, and abundant blood flow, whereas benign masses typically exhibit hyperechogenicity, regular morphology, and limited blood flow. Similar findings have been observed in this study as well as previously published studies [14], indicating that US can to some extent differentiate the benign and malignant nature of masses. However, not all masses have typical manifestations. For example, AML is a common benign mass with a lack of fat and manifests as a hypoechoic lesion on ultrasound examination. Moreover, malignant masses that are 30-60% small also exhibit hyperechogenicity [15]. In addition, malignant tumors with slow blood flow cannot display rich blood flow signals on conventional ultrasound.
CEUS is a pure blood pool contrast. The contrast agent is made up of phospholipid shell-stabilized gas microbubbles. These 3–7 micron microbubbles are small enough to squeeze past pulmonary capillaries and enter the arterial system but big enough to stay inside blood vessels. The distinction between benign and malignant renal tumors can be made more clearly with CEUS [16, 17] and enables the visualization of vascular perfusion inside the mass. In a meta-analysis of CEUS features in clear cell renal cell carcinoma with a diameter of less than 4 centimeters, Liu et al. [18] suggested that high enhancement has moderate sensitivity (67–89%) and specificity (42–75%), while rapid enhancement and uneven enhancement have high diagnostic ability (AUC of 0.74–0.84). However, unlike other organs in the body, the kidney has a small volume and a large blood flow, reaching up to 20 − 25% of the blood volume of the heart, indicating a high perfusion state. Research [19] suggests that the CEUS examination of renal cell carcinoma mostly demonstrates fast forward and fast backward under high enhancement; however, the majority of kidney tumors exhibit robust blood supply and lack excellent diagnostic specificity. Moreover, the quick perfusion of renal lesions during C-CEUS examination limits the capture of arterial blood flow information, hindering accurate disease diagnosis. By raising the acquisition frame rate, high frame rate contrast-enhanced ultrasonography (H-CEUS) enhanced temporal resolution of images and offered a superior evaluation of vascular enhancement, particularly microvascular enhancement, with upgraded temporal and spatial correlation resolution [20]. Our previous research confirmed that H-CEUS has high sensitivity (84.8%) and specificity (96.8%) in distinguishing between CCRCC and AML [21].
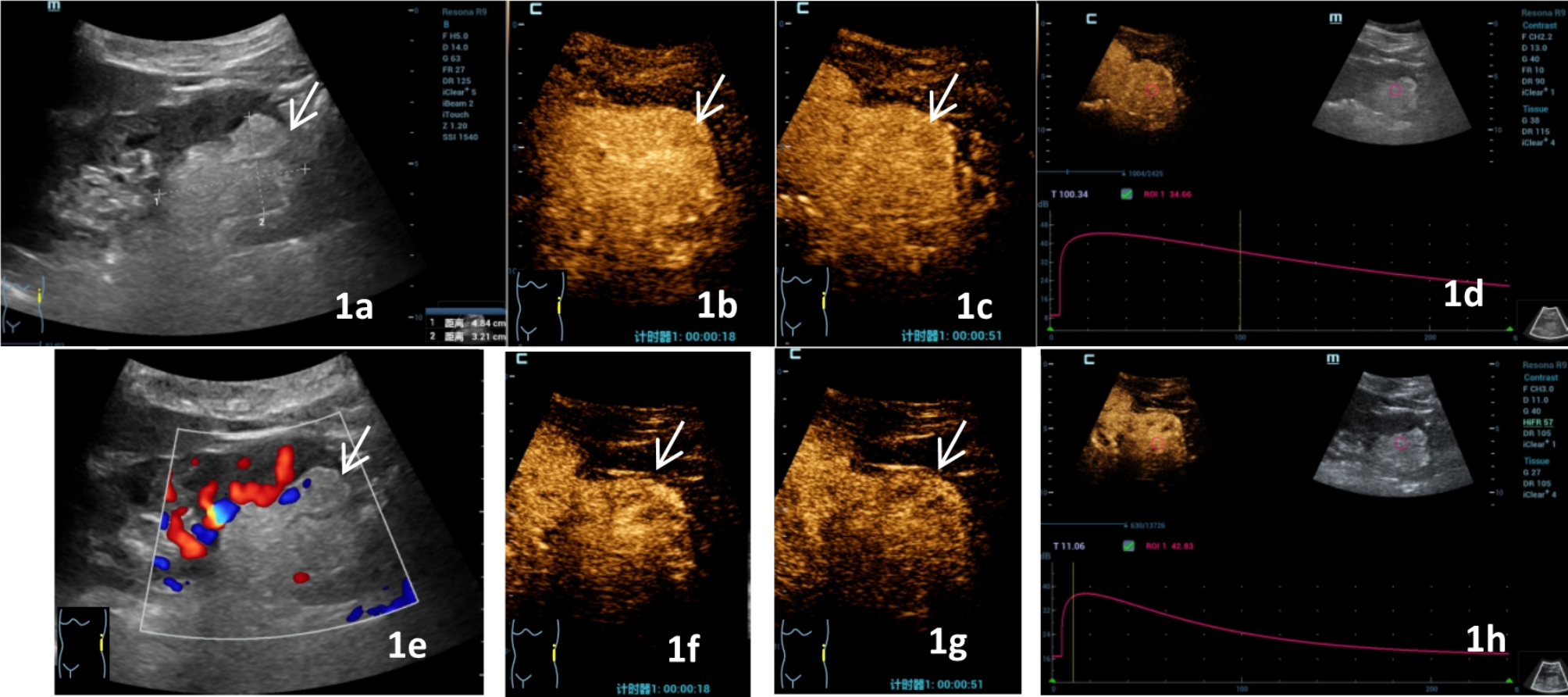
In the benign and malignant groups, two distinct contrast modalities of lesions were compared in this study. The results revealed statistically significant differences in the fill-in direction and wash-out mode of the two ultrasound modes in the malignant group (P = 0.041, 0.002). C-CEUS is mainly characterized by entirety enhancement, while H-CEUS is mainly characterized by centripetal enhancement. The difference in enhancement direction between the two contrast modes may be attributed to the increased frame rate, providing a clear image of the specific area of contrast enhancement that first appears inside the lesion. The expansion process of this enhancement area over time directly reflects the perfusion direction of the contrast agent. However, the specific location where the contrast-enhanced area first appears within the lesion cannot be accurately captured in cases with a low image frame rate. Rather, the contrast-enhanced region arises in different areas of the lesion almost simultaneously, resulting in a holistic perfusion effect. In addition, the presence of a large number of immature blood vessels and the higher rate of arteriovenous fistulas in malignant tumors provide oxygen and nutrients to the tumor, promoting tumor growth [22]. Therefore, both C-CEUS and H-CEUS exhibit rapid enhancement. However, the higher time resolution of H-CEUS can improve the frame rate of the image, display the blood flow characteristics of microvasculature more clearly, and improve the differentiating ability of the tumor [23,24,25]. Therefore, in this study, compared to C-CEUS, H-CEUS was found to more clearly display the initial peripheral enhancement of blood vessels and enhancement gradually move towards the center. Malignant tumors are nodules with abundant arterial blood flow perfusion, showing significantly faster perfusion compared to benign tumors. In addition, H-CEUS can detect the rapid movement of blood flow in arteries within the full field of view. Nonetheless, the benign nodule group did not exhibit a statistically significant variation in the enhancement direction between the two contrast modes. This could be as the benign nodule has fewer blood vessels and a sluggish blood flow perfusion, resulting in both C-CEUS and H-CEUS being able to display its perfusion process.
In malignant tumors, H-CEUS shows rapid wash-out, which is different from the slow wash-out of C-CEUS. The difference in wash-out might explained by the malignant tumors’ abundant blood supply, which requires a longer wash-out time. However, owing to the low frame rate of C-CEUS, the observed initial wash-out time does not reflect the true wash-out time point of the contrast agent inside the tumor. However, H-CEUS can more accurately observe the initial wash-out time of the contrast agent inside the tumor. In benign tumors, due to the limited number of blood vessels, fewer contrast agent microbubbles enter, resulting in poor contrast with the surrounding heterogeneous tissues. However, H-CEUS can display microvessels more clearly, providing a clear contrast with the surrounding necrotic tissue. In addition, In contrast to the surrounding normal renal cortex, which showed equal wash-out in five cases of C-CEUS, the malignant group’s H-CEUS wash-out pattern could be differentiated from it. This could be caused by the substantial improvement in temporal resolution and increase in image information brought about by the switch from 10 Hz in C-CEUS to 50–65 Hz in H-CEUS image capture and frame rate. Especially, H-CEUS reduces contrast agent damage, thereby extending its duration in the late stage and facilitating the observation of the fading mode [26].
The results of this study revealed that in the benign group, only the enhancement homogeneity showed a statistically significant difference between the two contrast modalities (p = 0.004), with the benign nodules in C-CEUS showing mainly homogeneous enhancement (21/30, 70.00%), and heterogeneous enhancement (20/30, 66.67%) in H-CEUS mode. This finding may be attributed to benign renal tumors tending to have fewer microvessels and slow flow within them, which are less likely to merge with liquefaction and show homogeneous echoes and homogeneous perfusion of the C-CEUS contrast medium. Nonetheless, by raising the frame rate, the first appearance of contrast enhancement within the lesion can be clearly seen, as well as the direction of contrast agent perfusion and blood flow perfusion; which changes over time and reduces the error of contrast-enhanced ultrasound imaging [27], resulting in the hermogeneous enhancement of the benign group in the H-CEUS mode.
In the TIC parameter analysis of this study, the PI of C-CEUS was higher than that of H-CEUS in both the malignant and benign groups. Moreover, a lower number of contrast microbubbles was accommodated by H-CEUS in the same sampling frame, with a shorter residence time, leading to a lower PI value than that of C-CEUS. Similarly, the higher temporal resolution of H-CEUS enabled accurate observation of the time of entry of contrast microbubbles into the mass and the time of exit. In addition, this duration can be narrowed down, resulting in lower MTT and DT/2 in H-CEUS compared to C-CEUS in both the benign group and the malignant group. Furthermore, the AUC was significantly lower in H-CEUS compared to C-CEUS. In addition, the H-CEUS TIC parameter AS was higher than C-CEUS in the malignant group, and the elevated AS manifested as a steeper and straighter ascending branch of the TIC curve. These results may be attributed to the difference between H-CEUS and C-CEUS; the former had a high frame rate and strong temporal resolution, providing detailed information on the perfusion period of the renal contrast [21]. Malignant renal tumors tend to be blood-rich supply foci, resulting in rapid entry of the contrast agent. In contrast, C-CEUS has a low frame rate and cannot accurately display the contrast agent perfusion process. However, the H-CEUS mode improves the number of image acquisitions from 10 Hz in C-CEUS to 50–65 Hz in H-CEUS, which greatly improves the temporal resolution, enhances image information, and more accurately responds to the process of TIC curve rise.
Nonetheless, the shortcomings of the present study should be acknowledged. (1) The sample size of patients was limited. This study solely examined benign and malignant renal tumors, without grouping renal cancers with different pathological classifications. (2) The study concluded a correlation between tumor size and contrast perfusion process. However, tumor size was not grouped in this study. In the future, the sample will be further expanded and grouped for renal tumors of different classifications and sizes to further clarify the advantages of the application of HFR CEUS. (3) Prospective studies are required to further evaluate the clinical value of H-CEUS technology in the differential diagnosis of the nature of renal tumors.


Comments (0)