AIM is a group of self-limiting fundus disorders characterized by the sudden onset of central vision loss in young people. The etiology of AIM remains unclear, with increasing reports linking the disease to viral infections [9, 10]. We conducted a review of over 90 cases reported between 1991 and 2023. In 78% of the cases, patients presented with influenza symptoms prior to ocular symptoms, while 43% had fever, 22% had sore throat, and 12% exhibited rash maculopapulars. However, around 30% of patients did not display influenza-like prodrome or test positive for viral antibodies, indicating potential involvement of autoimmunity in the pathogenesis of AIM. Meanwhile, it suggests that reliance solely on evidence of past infection in diagnosis should be avoided.
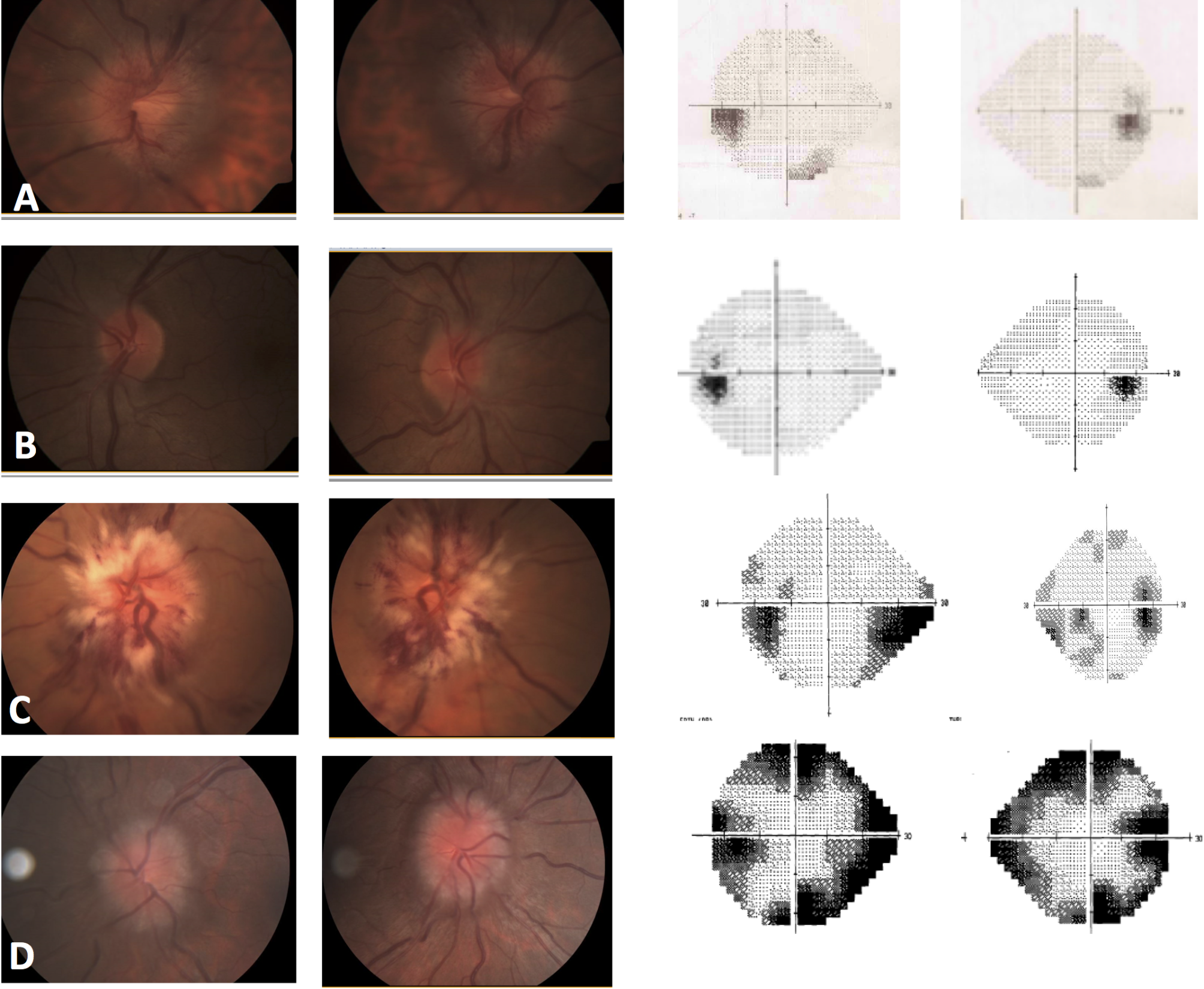
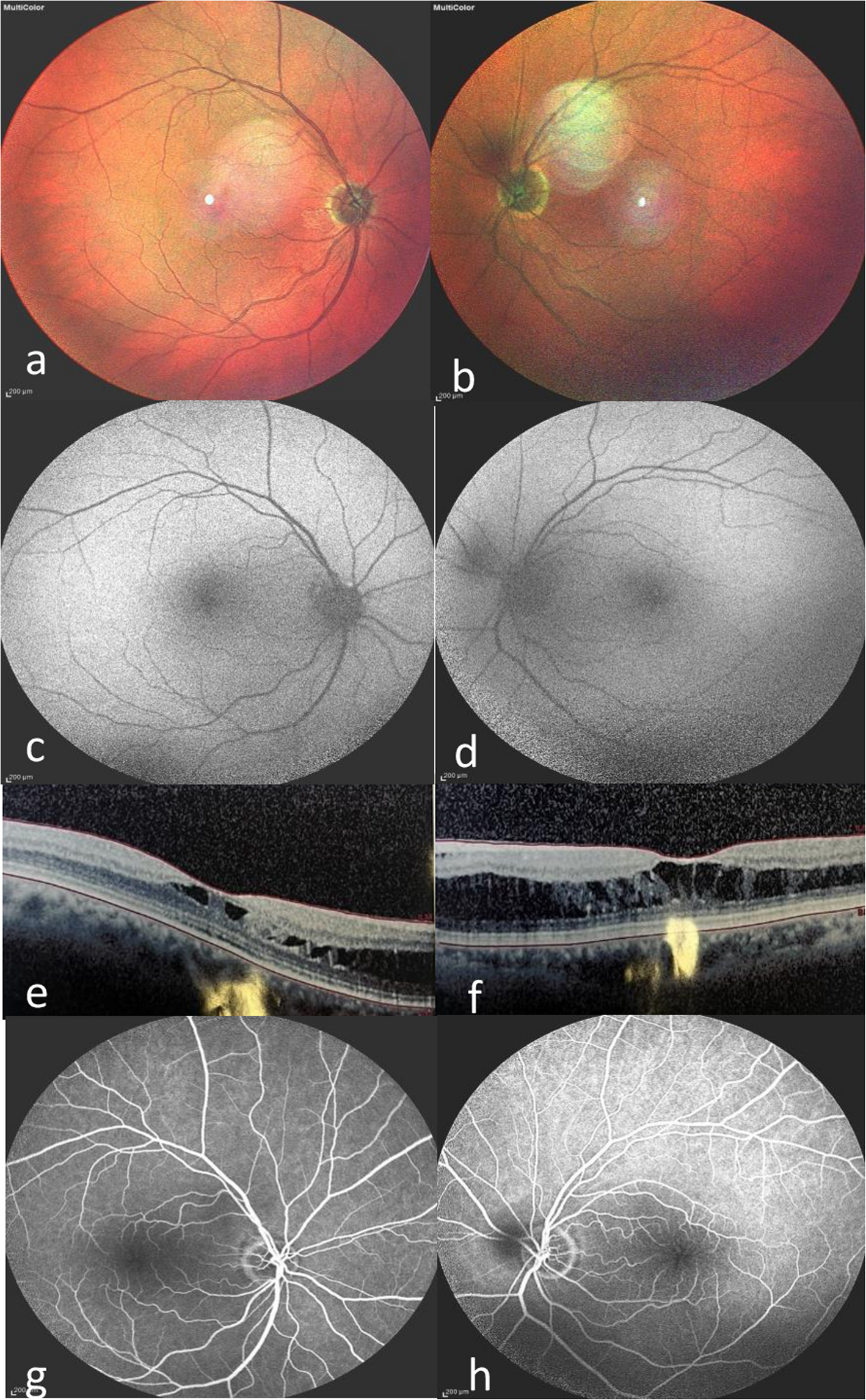
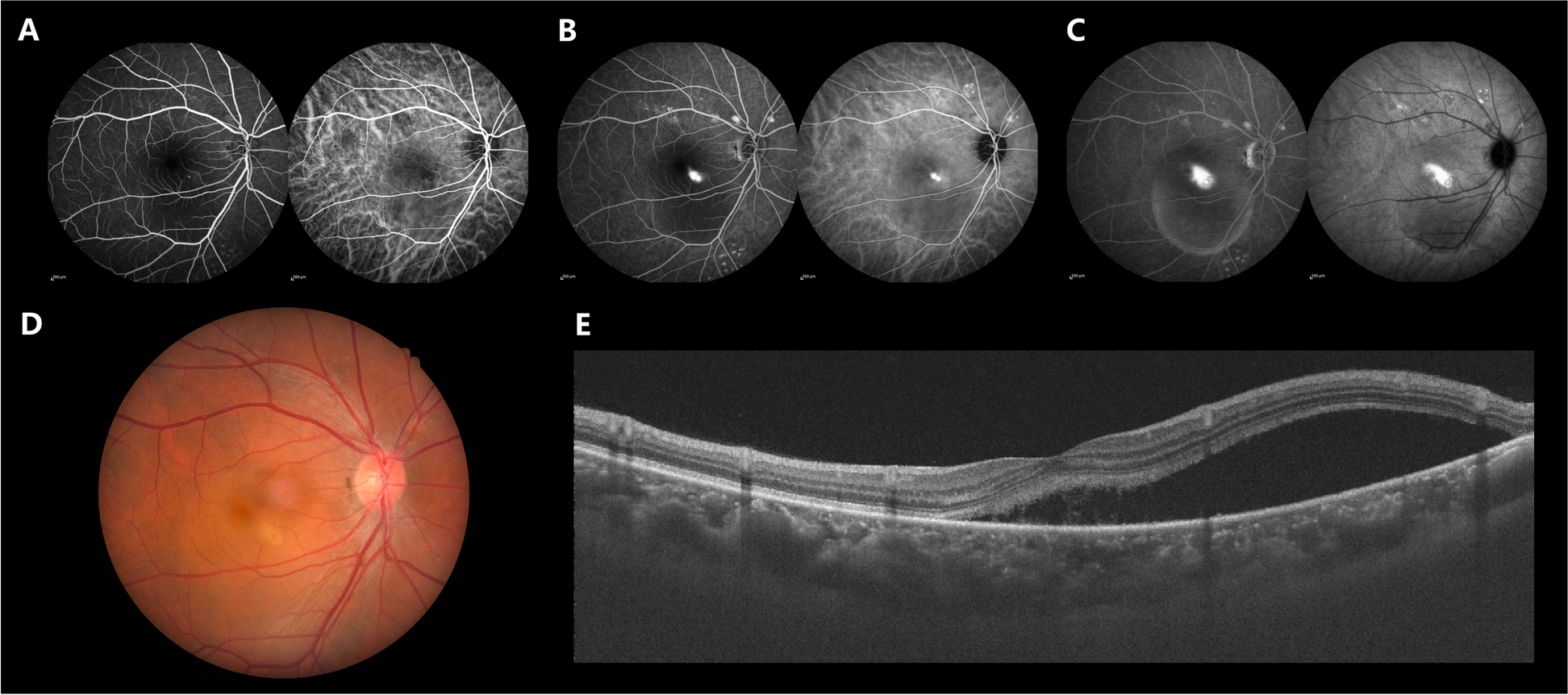
In the initial stage, the fundus appears as yellowish white subretinal exudate or hypopigmentation halo in the macular area, and may also be accompanied by bleeding at the detachment of the retinal nerve epithelium. Optical Coherence Tomography (OCT) shows retinal plasma detachment, ellipsoidal band discontinuity, and significant thickening of the choroidal. OCTA shows decreased blood flow velocity in the deep capillary complex and choroid. Fluorescein fundus angiography (FFA) demonstrated hypofluorescent alterations in the region of initial plasmacytoid retinal detachment, hyperfluorescence encircling the periphery of the lesion in the intermediate stage with prolongation of time, and discoidal intense fluorescence due to fluorescein accumulation in the late stage. Early and late ICGA shows low fluorescence corresponding to AIM lesions. Autofluorescence (AF) reveals locally enhanced hypo-autofluorescence in the center recess, corresponding to intraretinal hemorrhage as shown on funduscopy. Recovery occurs after 3–6 weeks when the inflammation subsides and the plasma retinal detachment resolves on its own. On fundus imaging, the central highly pigmented RPE is surrounded by a “necklace” of hypopigmented areas, forming a typical “bull’s-eye” appearance. The OCT scan revealed a return to normal retinal structure, with some residual disruption or thinning of the photoreceptor layers and a significant reduction in choroidal thickness. Additionally, OCTA demonstrated a marked increase in choroidal blood flow velocity.
There was a temporal relationship between the development of flu-like symptoms and vision loss in our patient. Despite the lack of early ICGA monitoring, late normalcy suggests a return of vascular function, consistent with the natural course of AIM. With similar fundus images, OCT, FFA, and AF manifestations, the diagnosis of AIM was established. Unlike previous cases, this patient is older and is the sixth case of binocular episodes following the previous reports, with a high degree of symmetry in both her eyes.
In this case, the hypersensitive CRP level was notably elevated at 172.63, accompanied by a decrease in lymphocytes and an increase in monocytes during the early stages of the disease, collectively indicating a likely viral etiology for the patient’s fever. Additionally, abnormalities in partial thromboplastin time, thrombin time, fibrinogen levels, and D-dimer suggest a state of hypercoagulability. Notably, this patient presented with multiple areas of nonperfusion in the peripheral retinal region, a pathologic change that has rarely been reported in previous cases, which reflects the pathology of retinal microcirculatory dysfunction. Firstly, we hypothesized that the direct destruction of vascular endothelium due to inflammation could be a common etiological factor underlying this pathological alteration and subretinal fluid accumulation. Secondly, impaired microcirculation may be the result of immune complex deposition, which supports the role of the immune response in AIM. In addition, in an imaging study of COVID-19-associated acute macular neuroretinopathy, Bin et al. concluded that infection induces an overactive immune response and “cytokine storm” which result in microvascular damage [18]. Such damage triggers a decrease in the density of deep capillary blood flow. The macular cystoid edema may resolve as vascular function recovers and inflammation subsides; however, occlusion of the peripheral retinal capillaries may persist due to irreversible vascular damage. C-reactive protein (CRP) is an acute phase reactant to infection and is widely used in clinical practice as a marker of infection or inflammation. It has been suggested that CRP may promote thrombosis through multiple channels, including inducing monocytes to express procoagulant tissue factor (TF) [19], increasing levels of E-selectin, vascular hemophilic factor, IL-6, IL-8, serum amyloid A, type II secreted phospholipase A2, plasminogen, and D-dimer in blood circulation, and activating inflammation and coagulation [20]. And the correlation between c-reactive protein and the development of atherosclerosis and thrombosis has been widely recognized [21]. Van Hecke et al. showed that high serum levels of CRP are associated with the development of diabetic retinopathy [22]. Diabetic retinopathy is a retinal vascular disorder characterized by diverse fundus manifestations, which may also present as retinal microvascular occlusion and macular edema like AIM. Its onset and progression are closely associated with abnormal oxidative stress [23], indicating that inflammatory factors such as CRP and vascular endothelial growth factor (VEGF) may play a role in the pathogenesis of AIM. All of the above support the destruction of the normal microvascular system by CRP, so the high CRP level in this patient may also be an explanation for the no perfusion in the peripheral retina. We believe the periretinal vascular occlusion is suggestive of the pathological mechanisms underlying this disease; however, its influence on prognosis warrants further investigation.
This disease needs to be differentiated from infectious exudative maculopathy due to antecedent flu-like symptoms. In cases of suspected AIM, it is important to exclude infections due to various causes. A thorough medical history and laboratory investigations are crucial for the accurate diagnosis. Because of the presence of peripheral retinal punctate haemorrhage and retinal vascular occlusion, tuberculosis infection was initially suspected to be the cause in this case, but the hematological examination did not support it and there were no pathological changes such as anterior uveitis, retinal vasculitis, serrated choroiditis, choroidal nodules, or tuberculous tumors, which often appear in ocular tuberculosis [24], therefore, it is excluded. Both acute retinal necrosis caused by herpesvirus infection and Behçet’s disease can present as retinal vasculitis. Nevertheless, in this case, the necrotic changes had not progressed, and there were no significant vitreous opacity, retinal artery thinning, thus acute retinal necrosis could be ruled out on this basis. The patient denied previous oral ulcers, vaginal ulcers and other lesions, and there is no retinal vascular fern-like fluorescence leakage on fluorescence angiography. On this base, Behçet’s disease was excluded. Other possible differential diagnoses to consider include central plasma choroidal retinopathy ( CSCR ). CSCR can present as acute vision loss with disc-shaped retinal detachment in the macular region, similar to this case; however, FFA can distinguish between the two based on their pathological mechanisms. In CSCR, disruption of the closed zonule between the retinal pigment epithelium causes fluorescein to leak in a “smoky” pattern during the acute phase of FFA and changes to an “ink-like” appearance in its chronic stage. The irregular early hyperfluorescence of AIM, the staining in the late retinal thickening, and the “lake-like” staining underneath the neurosensory retinal detachment are similar to the fluorescence of choroidal neovascularization (CNV), which can be differentiated by indocyanine green angiography if necessary. Distinguishing AIM from CSCR and CNV is critical because CSCR and CNV require aggressive and timely intervention to avoid potential threats to vision. Acute posterior segment multifocal discoid epitheliopathy (APMPPE) shares several features with AIM [25]. Both are prevalent in healthy young and middle-aged people, with acute vision loss after flu-like symptoms, grayish-white patchy lesions in the macula, similar FFA manifestations in the acute phase, and vision that mostly recovers on its own after remission. Therefore, many scholars believe that UAIM may be a type of APMPPE. In comparison, AIM changes are relatively mild and confined to the outer retina. APMPPE is mostly binocular, with multifocal lesions in the posterior pole. The typical bull’s-eye-like changes of AIM can also be one of the differentiating points.
Nakazawa et al. found persistent damage to photoreceptor cells after remission by performing multifocal electroretinography (mf-ERG) [26]. It was shown that the application of systemic steroids 1 mg/kg/day exhibited good visual recovery within one week [27]. However, unlike these studies, ROSAR et al. retrospectively analyzed 17 previous patients and found that the visual prognosis of the four patients treated with corticosteroids was not significantly different from that of the patients without intervention, and all patients’ vision was fully restored except for one patient who developed choroidal neovascularization during the follow-up period [28]. Singh’s case demonstrated a favourable response to non-steroidal anti-inflammatory drugs (NSAIDs), with a notable improvement in visual acuity observed after seven days of topical administration [29]. Furthermore, it has been proposed that vitreous injection of Abelacimab may facilitate disease regression by fostering the restoration of the blood-retinal barrier and anti-inflammatory effects [30]. However, further research is hindered by the challenge of differentiating between extrinsic intervention and the natural regression of the disease. Ultimately, there is no consensus on the optimal treatment for AIM, and the clinical efficacy of glucocorticoids, NSAIDs, and anti-VEGF agents remains confirmation in larger cohort studies.
Although AIM may have a natural course of visual recovery, its potential complications could lead to poor visual prognosis, such as outer retinal tubular structures, choroidal neovascularization, subcentral fibroepithelial metaplasia, macular hole, subcentral pigmentary degeneration, atrophic macula, neural retinitis, and retinal pigment epitheliopathy with hyperpigmentation and/or pigment loss [31, 32]. In our retrospective analysis of more than 90 cases reported from 1991 to 2023, 6 cases presented decreases in visual acuity twice after the first attendance, 3 of which were found to have CNV by fluorescein fundus angiography and ICGA. CNV with discoidal scarring is a nonspecific consequence of pigment epithelial disorders that can lead to permanent and severe loss of central vision [1], involving a variety of inflammatory cytokines as interleukin family and VEGF [33]. RPE not only contributes to the establishment of the blood-retinal barrier but also plays a crucial role in immune regulation. In response to inflammatory mediators such as TGF-β, RPE is capable of secreting various cytokines and VEGF [34]. Consequently, the impairment of RPE in AIM may lead to an increased risk of CNV. Therefore, it is suggested that when patients experience further vision loss, although it may be due to the natural course of the disease, it is also possible that complications such as choroidal neovascularization have developed, at which point further investigations, as well as pharmacologic or other forms of intervention, are necessary.




Comments (0)