This study provides novel insights into the clinical characteristics, prognostic factors, and treatment outcomes of MD in patients of South Korean descent, contributing to a deeper understanding of the disease within the Asian population. Our findings highlight the importance of early intervention, lipid management, and combination therapy in improving treatment outcomes for this challenging condition. Additionally, we were able to confirm the importance of monitoring the initial response after treatment.
One of the most significant findings of our study is the association between shorter symptom duration and better treatment outcomes. Patients who achieved TR had a significantly shorter mean duration of symptoms compared to those with PR. This suggests that early diagnosis and prompt initiation of treatment are crucial for managing MD effectively. The importance of early intervention in MD aligns with recent studies on chronic lymphedema and rosacea, which are considered underlying etiopathogenic factors of MD. For instance, Zhang et al. [20] demonstrated that prolonged exposure to LL-37, a peptide implicated in rosacea pathophysiology, results in irreversible dermal hyperplasia and persistent erythematous skin changes. Our findings support this concept, suggesting that early treatment of MD might prevent such irreversible changes, leading to more favorable outcomes [20, 21].
Another key finding of our study is the association between lower LDL-C levels and better treatment response. This novel observation suggests a potential link between lipid metabolism and MD pathophysiology or treatment response. The role of LDL in inflammatory skin conditions can be explained through its interaction with Toll-like receptors (TLRs), particularly TLR-2, which is elevated in rosacea-affected skin. LDL has been implicated in activating proinflammatory responses through TLR-2 signaling pathways. The association between high LDL levels and poor treatment response in our study suggests that the proinflammatory milieu enhanced by LDL might impede therapeutic efficacy in MD [22,23,24,25]. Recent meta-analyses have demonstrated a strong association between rosacea and cardiometabolic diseases, including dyslipidemia [26]. Our findings extend this concept to MD, suggesting that lipid management could be an important aspect of MD treatment.
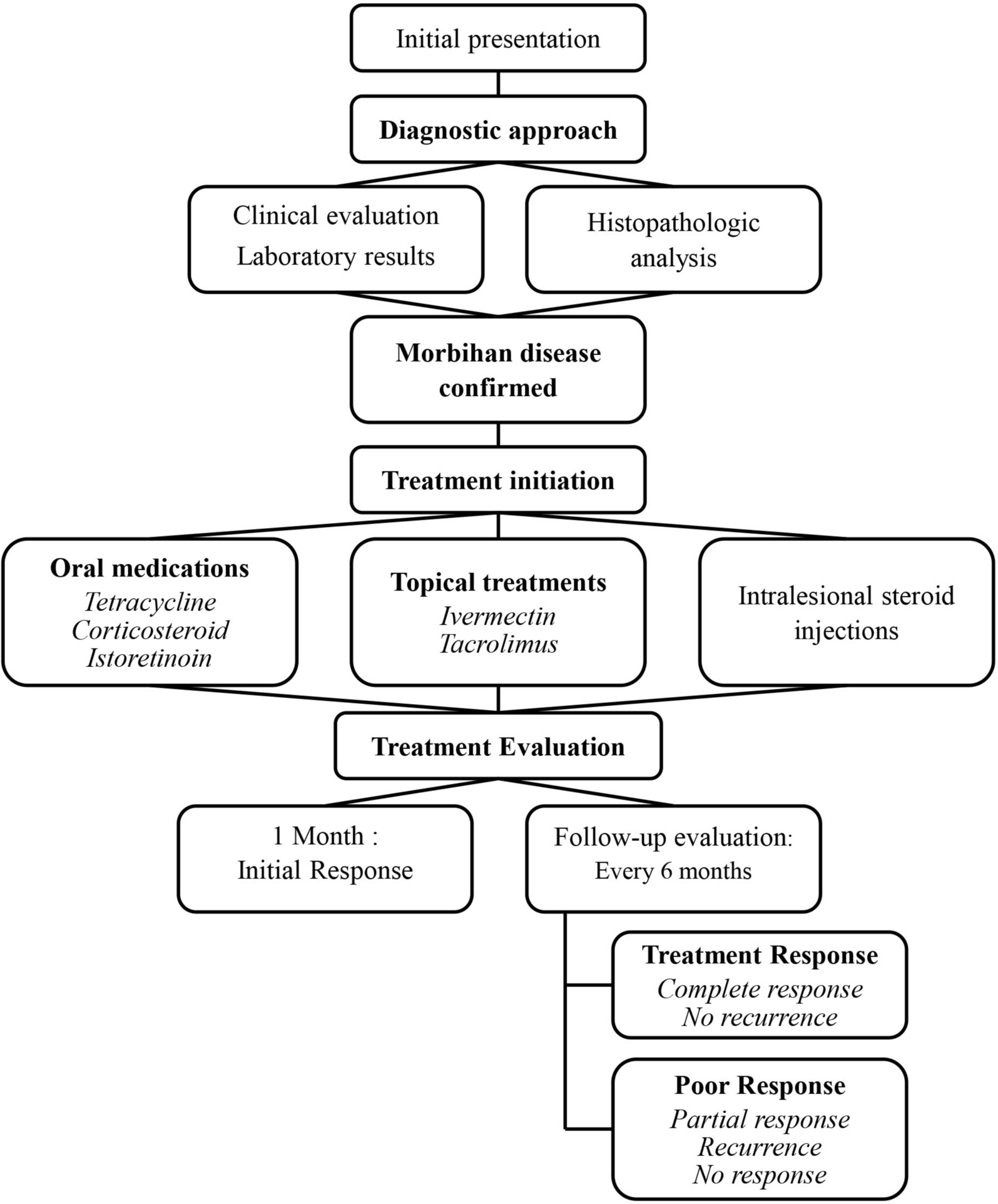
Previous reports on MD treatment have highlighted that combination treatment and long-term management are crucial to ensure a positive response. Mireille et al. [21]. reported that a longer treatment duration of at least 6 − 12 months was associated with more satisfactory results. Combining eyelid reduction surgery with intralesional corticosteroids, isotretinoin with ketotifen, and tetracycline with systemic corticosteroids may help control symptoms [21]. In contrast, some studies have found that combination therapies show no correlation with treatment response [5, 12]. In this study, the treatment methods were divided into three groups: (1) Oral medications (isotretinoin, tetracycline, or corticosteroids) only; (2) oral medications combined with topical medications (tacrolimus or ivermectin); (3) treatment with additional ILS injections [7, 13, 18, 19, 27, 28]. In more than half of the patients who showed TR at the 6-month follow-up, combination treatment with oral and topical medications from the initial treatment and during the treatment period was a significant factor in achieving complete MD remission. Moreover, our study found that partial treatment response at 1 month was significantly associated with complete remission at the final visit. This observation underscores the value of early treatment response as a prognostic indicator, which has not been previously reported in MD literature.
Mireille et al. [21] also reported that 80% of patients treated with isotretinoin showed a positive response, highlighting its effectiveness in managing MD. However, it is noteworthy that many of these favorable outcomes are derived from case reports, where selection bias may play a role in highlighting responsive cases. In our study, which included a more diverse sample with an entirely Asian cohort, the response rate was around 30%. Additionally, our treatment protocol differed, incorporating adjunctive therapies such as topical treatments (Protopic, Ivermectin) and ILS injections—absent in previous protocols—which may have influenced outcomes. These factors—case severity, patient population, and treatment protocols—likely contributed to the differences in response rates observed between the studies.
The histopathological findings in our study, particularly the prevalence of perivascular or perifollicular lymphocytic infiltration, are consistent with previous reports [5, 11, 14, 28]. This was followed by dermal edema, focal granulomatous infiltrations, and telangiectasia. Notably, Demodex, the main microorganism that triggers the inflammatory reaction in rosacea, was found in one case of MD. Although this does not prove a definitive link between MD and Demodex, it is significant as it marks the first study where Demodex was identified in histological examinations of an Asian patient with MD. These findings illustrate the diverse histopathological spectrum of MD and its complex diagnosis and treatment.
Our observation of ANA positivity in 50% of patients, albeit at low levels, challenges conventional diagnostic criteria that associate ANA negativity with MD [4, 5, 28]. This finding is particularly intriguing when considering that ANA positivity in healthy individuals can reach up to 40% using indirect immunofluorescence techniques [29]. While this prevalence aligns with general population data, it suggests a need for a more nuanced approach to MD’s immunological profiling. Additionally, ANA is known to be present in over half of rosacea patients, which supports the idea that Morbihan disease may share a similar disease spectrum with rosacea [30]. This contrasts with previous studies that reported ANA negativity in MD, highlighting a potential area for reconsidering and updating the diagnostic criteria for MD. The presence of ANA in our study, without corresponding systemic or connective tissue diseases, underscores the potential for a more intricate immunological environment within MD than previously recognized.
The partial and variable responses to established treatments, such as tetracycline-based antibiotics, corticosteroids, and isotretinoin, present challenges for clinicians and patients. Our research indicates a trend towards improved outcomes with combined therapeutic approaches, potentially owing to a multifactorial impact on various pathogenic mechanisms in MD. The use of tacrolimus ointment, which acts in a manner similar to that of macrolide antibiotics, has emerged as a potentially effective component of combination therapy [27, 31]. Although not statistically significant, this finding suggests an anti-inflammatory effect worthy of further exploration.
It is crucial to acknowledge the limitations inherent in our study design. The retrospective nature and relatively small sample size may have introduced bias and limit the generalizability of our results. Additionally, the absence of a control group constrains our ability to definitively assess the long-term durability of treatment responses. Despite these limitations, our study offers valuable insights that have significant implications for both future research directions and clinical practice in MD management.
The identification of early symptom duration and LDL cholesterol levels as potential prognostic factors represents a notable advance in our understanding of MD. These findings not only provide tangible targets for clinical assessment but also raise intriguing questions about the underlying pathophysiology of the disease. The apparent link between lipid metabolism and MD outcomes suggests a previously unexplored avenue of research. Future studies investigating the relationship between lipid profiles, lymphatic dysfunction, and MD progression may reveal novel therapeutic targets and preventive strategies. Furthermore, the relationship between combination treatment regimens and early treatment response as factors for TR provides an important strategy for treatment approaches in patients with MD.




Comments (0)