In this study, we used bidirectional TwoSampleMR analysis to investigate the causal relationship between RA status and immune cell measurements based on publicly available GWAS data. We first used 731 immune cell phenotypes as exposure factors and RA as the outcome factor. Immune cell phenotype classification was crucial in this study and mainly consisted of four types: AC, MFI reflecting surface antigen levels, MP, and RC. These molecules are typically detected by staining or fluorescence labelling, resulting in measurements of MFI and RC, which represent the density and expression levels of surface markers on immune cells, respectively [31]. Cell population counts play an important role in the immune system, and therefore, their quantity and status are critical for normal immune system function. Cell population counts are typically categorized into RC and AC, where RC indicates the percentage of a specific type of immune cell in the total cell count in a sample, and AC refers to the actual number of a specific type of immune cell in each volume of sample [32]. The activity of immune cells includes their role in the immune response as well as the cytokines and other molecules they produce. These activities can be determined by analysing cytokines secreted by immune cells or cell apoptosis [33]. The morphological features of immune cells, such as size, shape, and colour, are also included. These parameters can be used to monitor morphological changes in different types of immune cells in the immune system and provide useful information for diagnosis and treatment. Morphological parameters include aspects such as cell size, shape, number of cell nuclei, and chromatin morphology, which are usually observed by microscopy and counted manually [34]. By using these immune cell phenotype classifications, we can classify immune cells more precisely and summarize our results more accurately.
We identified 42 immune cell phenotypes that are causally related to RA, with the majority being MFI-based immune cells, totalling 33 different types. The MFI is a measure of the expression level of cell surface markers in immune cell research. By evaluating the fluorescence signal intensity, the MFI reflects the relative abundance of markers and can provide researchers with information on immune status, function, and responsiveness. Comparing the MFI values of different types or subtypes of immune cells can reveal differences in the expression of specific immune-related proteins. For example, in the study of T-cell subsets, comparing the MFI values of specific markers in CD4+ and CD8+ T cells can reveal their different roles and functions in immune responses [35]. In addition, MFI values can also be used to evaluate the function of immune cells. In inflammatory reactions, the expression of certain cell surface receptors may be upregulated, resulting in an increase in the MFI of the corresponding marker [36]. This phenomenon suggests that the cells are in an active immune response state and regulate the expression of markers to achieve their function. By detecting changes in the MFI values of specific markers, we can also evaluate immune cell responsiveness to external stimuli. When immune cells are stimulated by activators, the MFI of specific markers may increase, reflecting the sensitivity and activity of the cells to the stimulus [33]. Analysing the MFI values of specific markers in immune cells can provide important information about their biological characteristics, immune status, function, and responsiveness, which is crucial for understanding the underlying mechanisms of diseases and providing guidance for drug development and immunotherapy.
According to the analysis of 42 positive immune cells, 22 immune cells promoted RA, while 20 immune cells had a protective effect against RA. Through data analysis, it was observed that most of these immune cells belonged to two categories: the CDC group and the myeloid cell group. This finding suggested that these two types of immune cells play crucial roles in promoting the development of RA. CDC group cells, which act as antigen-presenting cells, are capable of capturing and presenting antigens to T cells, thereby initiating a specific immune response. On the other hand, myeloid cells, such as macrophages and neutrophils, are involved in inflammatory responses and joint destruction processes. The interplay between CDC group cells and myeloid cell group cells in RA is complex and diverse. Studies have revealed that in patients with RA, abnormal activation and excessive proliferation of CDC group cells may lead to imbalanced immune responses and tissue damage [37]. Moreover, myeloid cells also participate in the inflammatory response and cytotoxicity in RA, promoting disease progression through the release of inflammatory cytokines and the modulation of T-cell function [38]. Furthermore, the interaction between CDC group cells and myeloid cell group cells may also influence disease development and therapeutic outcomes. In recent years, advanced techniques and model systems have gradually unveiled the molecular mechanisms and interaction networks of CDC group cells and myeloid cell group cells in RA [39]. Therefore, we speculate that the interplay between CDC group cells and myeloid cell group cells in rheumatoid arthritis is intricate and intimate. They participate in the development and progression of RA through pathways involving immune response regulation, the inflammatory response, and joint destruction. Further research will contribute to a deeper understanding of the functions and interaction mechanisms of these cellular components.
In RA, protection against the disease is closely related to the maturation stages of T cells and monocytes, which are two important types of immune cells. T cells are a critical component of the immune system and undergo several key maturation stages, including positive selection, negative selection, and maturation. Abnormalities in T-cell positive and negative selection processes in RA may lead to an increase in autoreactive T cells and attacks on self-tissue. Recent research suggests that therapeutic strategies targeting T cells focus on inhibiting their abnormal activation and proliferation by modulating their signalling pathways and immune checkpoints, such as inhibiting the costimulatory pathway of T-cell activation and regulating T-cell activity through immune checkpoints such as CTLA-4 and PD-1 [40]. Monocytes are an important type of immune cell that differentiates into mature dendritic cells and macrophages in the bone marrow, both of which are involved in regulating immune responses. In RA patients, the activation and differentiation of monocytes may be abnormally stimulated by certain factors. These activated monocytes can produce sufficient levels of inflammatory factors, which can trigger the development and progression of arthritis. Studies have shown that the numbers and activity of mature dendritic cells and macrophages are significantly increased in RA, leading to synovial inflammation and cartilage damage [41]. Therefore, therapeutic strategies targeting monocytes mainly focus on inhibiting monocyte activation and differentiation. TNF-α and IL-6 are important inflammatory factors in RA, and their overexpression can cause abnormal monocyte activation. The inhibition of monocyte activation and differentiation through the regulation of these factors can achieve the goal of treating RA [42]. We speculate that controlling the normal forms of these two types of immune cells and inhibiting their abnormal activation and differentiation are important means of preventing the development of RA, as our research results have verified.
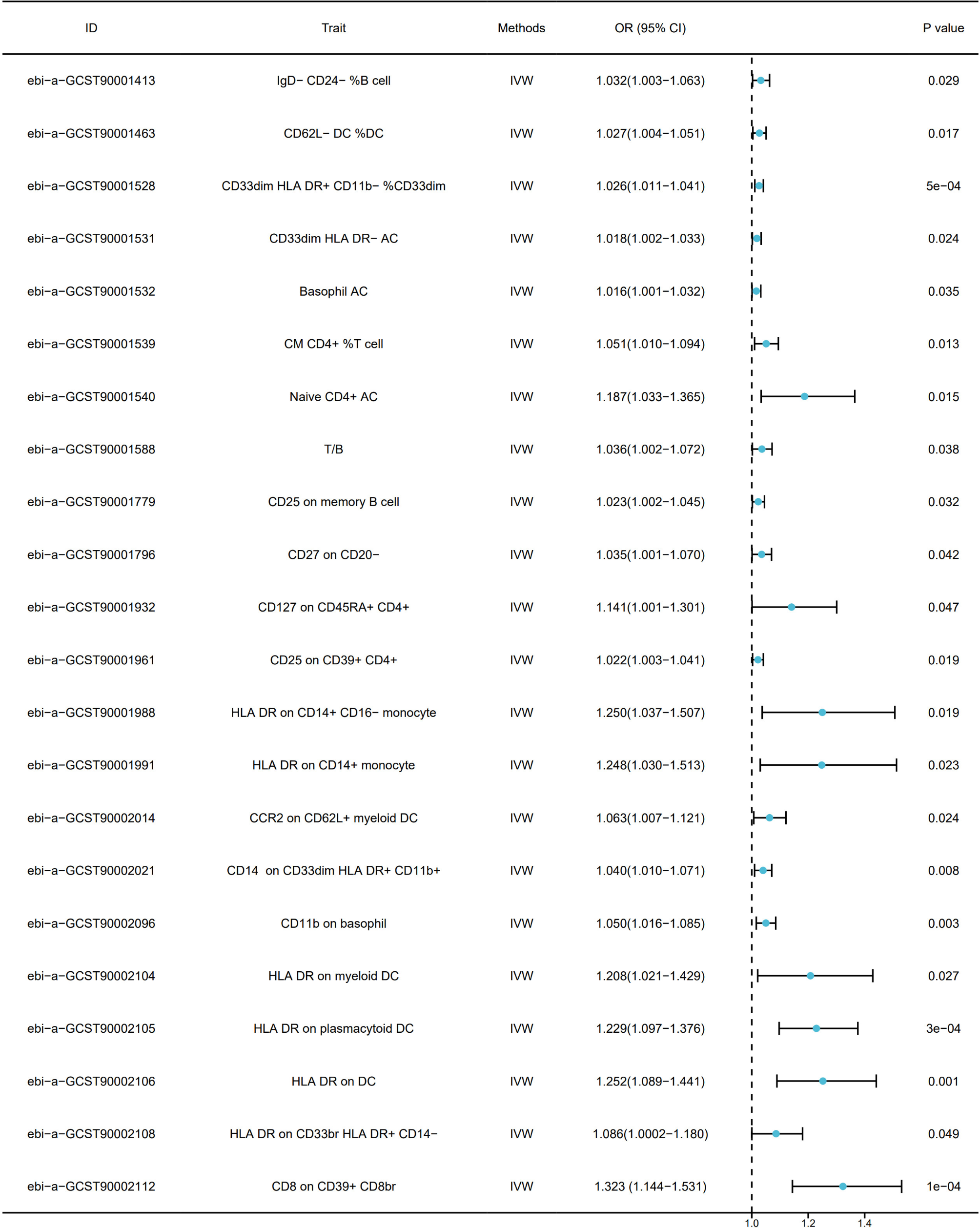
When performing reverse MR, we used RA as the exposure factor and focused on 42 types of immune cells as outcomes. Through our analysis, we found that there is a causal relationship between the onset of RA and the phenotypes of seven immune cells. Of these, RA and six of the cell types had a positive causal relationship, while one cell type had a negative causal relationship. The seven immune cell types we identified through bidirectional TSMR suggest that there is an important connection between the onset of RA and these immune cells. We were surprised to find that the immune cells with a positive causal relationship were concentrated on HLA-DR marker molecules, specifically HLA DR on CD14+ CD16- monocytes, HLA DR on CD14+ monocytes, HLA DR on myeloid DCs, HLA DR on DCs, and HLA DR on CD33br HLA DR+ CD14− immune cells.
HLA-DR is a member of the major histocompatibility complex (MHC) class II family. It is widely expressed on the surfaces of immune cells and plays an important role in regulating immune responses. HLA-DR molecules are closely associated with antigen presentation and T-cell activation. In patients with RA, specific alleles of the HLA-DR gene are closely correlated with susceptibility to RA [43]. HLA-DR molecules present joint-related antigens to CD4+ T cells, activating and perpetuating autoimmune reactions that lead to joint inflammation [44]. Additionally, HLA-DR molecules are involved in regulating the function and activity of immune cells. The synovium of RA patients contains many monocytes and macrophages expressing HLA-DR molecules. These immune cells interact with T cells through the expression of HLA-DR molecules, enhancing inflammatory responses [45]. Furthermore, HLA-DR molecules can regulate antigen presentation by immune cells and promote the production of proinflammatory factors, further exacerbating the development of joint inflammation. Therefore, interfering with the interaction between HLA-DR molecules and T cells can inhibit the inflammatory response and the process of autoimmunity. Other studies have shown the potential therapeutic effects of using antibodies against HLA-DR molecules to block their binding to T cells in the treatment of RA [46]. Further research on HLA-DR molecules is likely to reveal a very important drug target for the treatment of RA, which is consistent with our research results.
The only bidirectional causal association found to have a protective effect was CD4 on CM CD4+ immune cells, which likely implies its protective role in the pathogenesis of RA. CD4 on CM CD4+ cells, as crucial immune protective cells, possess high proliferative capacity and diversity, allowing them to differentiate into various effector T-cell subsets, such as Th1, Th2, and Th17, all of which play important protective roles in RA development. Additionally, CD4 on CM CD4+ cells exhibits memory properties, enabling rapid initiation and generation of more robust and persistent immune responses, which may contribute to RA relapse and progression. However, there remains considerable controversy and ambiguity regarding the specific relationship between CD4 on CM CD4+ cells and RA. Some studies suggest that alterations in the quantity and functionality of CD4 on CM CD4+ cells, such as reduction, abnormal activation, or functional impairment, may be associated with disease progression and severity [47]. Conversely, other studies have proposed the opposite, indicating a protective role of CD4 on CM CD4+ cells in RA, as they are capable of suppressing inflammatory reactions and joint destruction [48]. Nevertheless, our study supports the latter perspective, as we speculate that a comprehensive understanding of the specific mechanisms underlying the role of CD4 on CM CD4+ cells in RA will contribute to a better understanding and treatment of this complex autoimmune joint disorder.
MR is a causal inference method based on genetic instrumental variables that significantly facilitates the discovery of causal relationships between biomarkers and diseases, providing valuable insights for clinical practice. This approach not only supports the identification and validation of biomarkers, the formulation of personalized medical strategies, and the development of new drugs but also contributes to disease prevention, clinical guidelines, public health policies, and optimization of clinical research design, providing more accurate evidence for genetic counselling and thus promoting progress in the medical field and optimization of clinical practice. However, this method also has some limitations. First, GWAS relies on GWAS to identify genetic variants associated with specific exposure factors and is thus limited by the sample size and quality of GWAS. Insufficient or poor-quality data may lead to misidentification of genetic variants [49], thereby affecting the results of MR analysis. In addition, the core assumption of MR analysis is that genetic variants affect disease outcomes only through exposure factors, but there may be unconsidered confounding factors in reality, leading to bias. Moreover, genetic variants may affect disease outcomes through multiple pathways, i.e., through pleiotropy, further complicating causal inference. Moreover, since the impact of individual genetic variants on disease risk is usually small, MR analysis may suffer from insufficient statistical power, potentially resulting in false-negative results. Additionally, MR analysis is typically based on existing datasets, which may not contain information on certain emerging exposure factors, thereby limiting the applicability of the analysis. Furthermore, factors such as linkage disequilibrium and population stratification may also affect the results of MR analysis. Last, the complexity of biological processes may lead to nonlinear relationships between genetic variants and diseases, posing a challenge to MR analysis. Researchers need to exercise caution when interpreting MR analysis results and integrate other research evidence to obtain more reliable causal inferences [50]. To more accurately determine the causal relationship between two variables, multiple methods should be used for cross-validation to comprehensively consider different types of evidence.



Comments (0)