
Remember me


Early diagnosis and treatment are necessary for TAK to prevent irreversible damage to blood vessels. Therefore, appropriate imaging examinations are important (Fig. 1). A summary of the recommendations, level of evidence and degree of agreement for each elaborated clinical question is presented in Table 4.
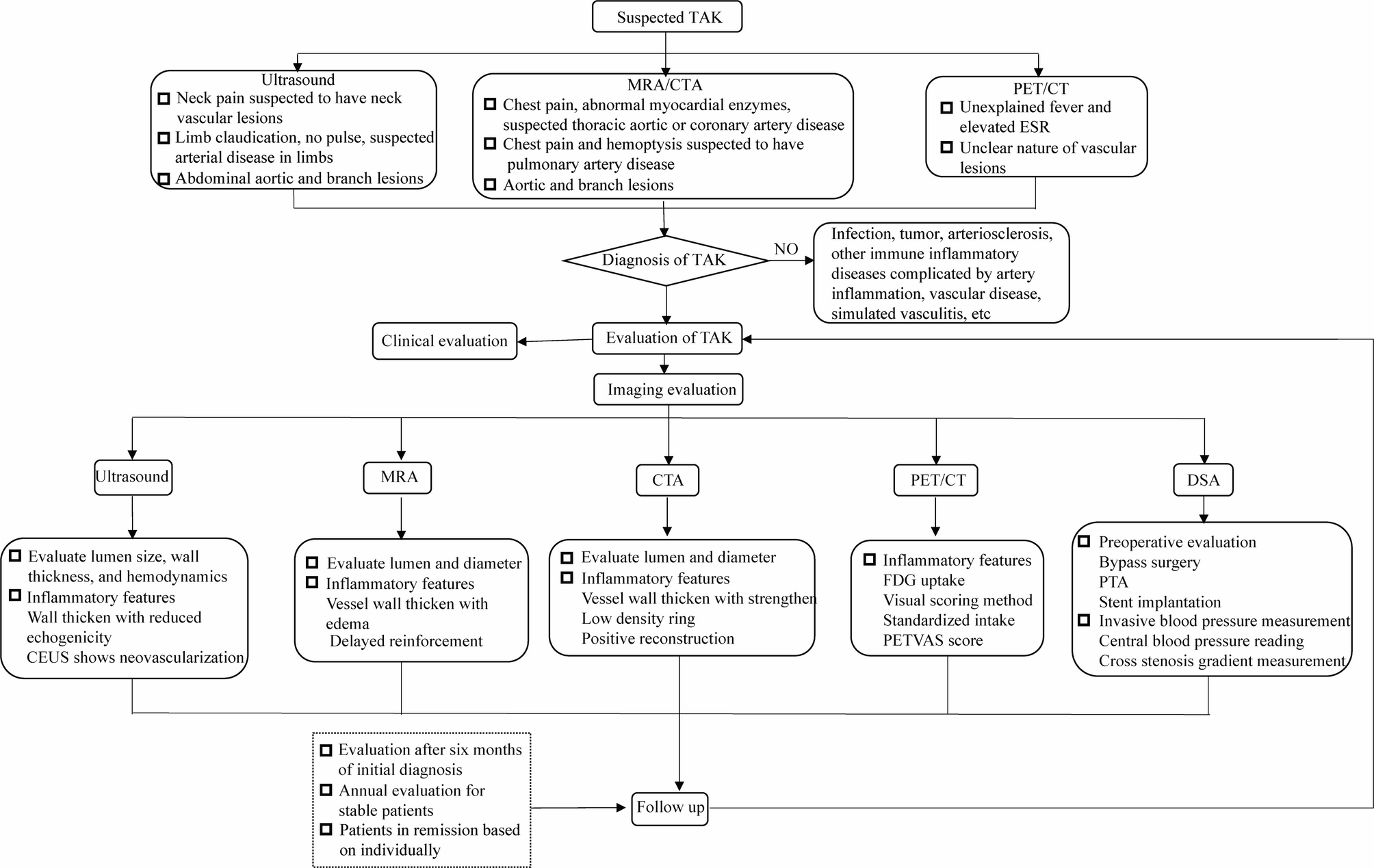
Fig. 1
Flowchart for the imaging diagnosis and evaluation of Takayasu arteritis
Table 4 Recommendations for the imaging diagnosis and evaluation of Takayasu arteritisClinical question 1: Imaging selection for patients suspected of having TAKRecommendation 1: DSA was the radiological gold standard for diagnosing TAK, but it has been replaced gradually by non-invasive and equally efficient imaging methods. Ultrasound is valuable for carotid artery (CA) and arteries in the upper and/or lower limbs and is therefore the first choice for screening patients with neck pain and limb claudication. For the aorta and its branches, computed tomography angiography (CTA) or magnetic resonance angiography (MRA) is recommended. If the patient presents with systemic symptoms such as fever and fatigue, positron emission tomography/computed tomography (PET/CT) can be used to detect vascular-wall inflammation and affected areas, and clarify if tumors or infections are present (2 B).
The characteristics of vascular lesions in TAK include involvement of the aorta and its branches, multiple vascular lesions, thickening of the circumferential wall of the annulus, inflammation of the vessel wall, and narrowing or dilation of the lumen. DSA is not sensitive to early wall lesions of the aorta or its branches (which may delay the diagnosis of TAK) and is invasive. Ultrasound has been used widely in the clinical diagnosis of TAK. Ultrasound can be selected if the patient has neck pain, cold hands, numbness, lack of pulse, limb claudication, or other suspected arterial lesions in the neck and limbs. The descending thoracic aorta is often involved in patients with TAK, but conventional ultrasound cannot be used to detect it. For patients suspected of having thoracic and abdominal aortic involvement, a comprehensive analysis of clinical manifestations, physical signs, and ankle–brachial index of blood pressure in limbs is needed [9], and CTA or MRA can be selected. For patients with chest pain and abnormal levels of myocardial enzymes, coronary CTA is recommended. For patients with chest pain, hemoptysis, and suspected involvement of pulmonary arteries on CT of the chest, then CTA of the pulmonary arteries is recommended. During the acute phase of TAK, CTA and MRA can be employed to detect wall thickening of the aorta and its branches before the appearance of abnormal luminal structures. For patients with non-specific manifestations, such as unexplained fever, increased ESR, and lack of vascular inflammation, PET/CT can be used to detect inflammation and lesions in the aortic wall, as well as infections or tumors. Adili et al. found that, during delayed PET/CT, the blood-pool activity of the inflamed lesions in the vascular wall was lower, and the uptake of 18F-fluorodeoxyglucose (FDG) was higher, thereby improving contrast of the lesions-to-blood pool and helping to detect wall inflammation [10].
Clinical question 2: Evaluation of systemic vascular imaging is required for patients with newly diagnosed TAKRecommendation 2: TAK causes multiple vascular lesions. The pathologic changes during the same period are diverse, including inflammation, scar repair, and thrombosis. Imaging can detect them in a timely manner. Therefore, comprehensive evaluation of imaging is important for diagnosis and comprehensive treatment. (5 D)
Patients with treatment-naïve TAK may have mild or limited clinical manifestations, which can lead to a missed diagnosis and inaccurate evaluation. Patients suffering from TAK have multivessel lesions, with type V being the most common in the 1996 Numano classification [11]. The vascular pathologic changes of TAK are complex and diverse, and imaging can detect vascular-wall inflammation and luminal lesions intuitively, which is an important basis for comprehensive treatment. Therefore, the Expert Group recommends that ultrasound, MRA, and CTA can be selected for systemic evaluation of vascular imaging for patients with treatment-naïve TAK.
Ultrasound has advantages for detection of the branches of the aortic arch, abdominal aorta and its branches, and limb arteries. MRA and CTA can image multiple parts of the chest and abdomen simultaneously, and can detect structural lesions in the walls and lumina of the aorta and its branches. Compared with ultrasound, the advantages of MRA and CTA are higher standardization of data acquisition, and MRA does not involve ionizing radiation. The speed of CTA is fast, but involves ionizing radiation. Hospitals with adequate facilities can carry out whole-body vascular examinations such as MRA or CTA. For hospitals that do not have adequate facilities, ultrasound can be used, or they can be evaluated at a higher-level hospital. Different imaging methods have their own advantages and disadvantages, and can be combined (if necessary) to optimize the diagnosis. Vascular assessment includes location, scope, structure (intimal, wall, perivascular tissues), nature (stenosis, occlusion, dilation, thrombus), severity, presence of inflammation, and hemodynamics [12].
Clinical question 3: Timing and frequency of image evaluation during follow-up of TAKRecommendation 3: In general, newly diagnosed patients should undergo imaging follow-up after 6 months of treatment. Patients with stable conditions should undergo imaging follow-up annually. For patients who require repeat examinations, ultrasound and MRA are recommended as first choices. For patients in clinical remission, the screening frequency and imaging methods used should be determined based on individual needs (5 D).
TAK is a difficult-to-treat disease. Therefore, through a series of imaging follow-ups and image comparisons before and after treatment, one can clarify the outcome of the original vascular lesions (lesion progression, unchanged or improved), whether there are new lesions, understand disease progression, treatment efficacy, or provide imaging evidence if clinical recurrence is suspected.
In many clinical studies evaluating the efficacy of drug treatments for TAK, MRA, CTA, or PET/CT were used to observe changes in vascular imaging from 6 months to 12 months after treatment [12,13,14,, 16].
It is recommended to undergo imaging examinations in four main situations: (1) increased serum levels of inflammatory markers without specific manifestations; (2) new ischemic events; (3) if disease-related ischemic manifestations worsen; (4) suspected clinical recurrence. Studies had found that positive imaging findings were more sensitive than clinical symptoms and detection of acute reaction protein [17, 18]. If clinical and laboratory test results are uncertain, imaging examinations can clarify clinical evaluation.
Clinical question 4: Imaging selection during the follow-up of TAKRecommendation 4: MRA, CTA, PET/CT, or vascular ultrasound can be used to evaluate vascular inflammation and monitor chronic structural changes at the site of vascular inflammation during follow-up. PET/CT is a sensitive form of imaging for monitoring vasculitis, but it is not recommended as the preferred method or for frequent short-term examinations (2 B).
The methods for imaging evaluation include ultrasound, CTA, MRA, and PET/CT, which are commonly used for assessing TAK activity and can distinguish disease activity from irreversible vascular damage [3]. One study involving 106 patients with TAK, with a median follow-up of 16 months, found that half of patients had recurrence according to the Kerr score [18]. However, the disease response rate was lower if evaluated by contrast-enhanced ultrasound (CEUS) of the CA, indicating that imaging assessment is more sensitive than clinical assessment. Two PET/CT studies showed that, after treatment relief from TAK, 18F-FDG uptake in the vascular wall improved, which could have reflected changes in disease activity during follow-up [19, 20]. One study involving 28 patients with TAK suggested that patients with high vascular uptake of 18F-FDG (maximum standardized uptake value (SUVmax) ≥ 1.3) had an increased risk of recurrence in the future [21]. Thickening of the vessel wall and narrowing of the lumen are common imaging manifestations of TAK, which may be manifestations of inflammation or post-inflammation repair, increased extracellular volume during scar formation, or diffused fibrosis [22, 23]. Therefore, disease activity cannot be evaluated based solely on these two manifestations. Hence, comprehensive evaluation of the clinical and imaging findings of inflammation is needed.
Diagnosis of TAK using ultrasoundClinical question 5: Ultrasound operators should receive professional trainingRecommendation 5: Vascular ultrasound should be undertaken by experienced ultrasound physicians or trained physicians. Standardizing instrument parameter settings and operating methods can help reduce the risk of operators deviating from standardized protocols (5 D).
Clinical question 6: Ultrasound diagnosis and characteristic manifestations of TAKRecommendation 6: Ultrasound images of TAK are characterized by diffuse circumferential thickening of the vessel wall, with or without changes in the lumen, and the characteristic feature is the “macaroni sign” (2 B).
Ultrasound two-dimensional imaging can detect changes in the arterial lumen and intima-media thickness (IMT), especially in the CA. Maeda was the first to describe the characteristic image of CA in TAK displayed by ultrasound, with diffuse circumferential thickening of the vessel wall, known as the macaroni sign [24]. One meta-analysis showed that, compared with clinical standards, the overall sensitivity and specificity for diagnosing TAK using carotid ultrasound IMT with a cutoff of 1 mm were 81% and 100%, respectively [25]. One study in 2023 found that arterial-wall thickening in patients with TAK led to increased arterial stiffness [26]. The sensitivity and specificity of shear-wave elastography (which uses the shear-wave velocity of ultrasound to evaluate the elasticity of biological tissues) for diagnosing TAK were 91.8% and 96.5%, respectively.
Clinical question 7: Ultrasound follow-up of changes in vessel-wall inflammation and lumenRecommendation 7: Diffused thickening of the vessel wall, reduced echo in the thickened area, and formation of neovascularization within the wall observed by contrast-enhanced ultrasound (CEUS) are signs of vessel-wall inflammation. Thickening of the intima is a sensitive indicator of inflammation. Intramural neovascularization is a specific manifestation of inflammation, and its efficacy in inflammatory evaluation is equivalent to that of PET/CT (2 B).
The IMT of the CA increases in patients with active TAK and decreases after treatment [16]. One meta-analysis showed that, using the Kerr score or physician’s global assessment (PGA) as the gold standard, the sensitivity and specificity of carotid IMT in diagnosing active TAK were 70% and 71%, respectively [17, 26,27,, 29]. Using the Kerr score as the gold standard, Seth et al. found that the sensitivity and specificity of diagnosing CA activity using IMT with a cutoff of 0.8 mm were 82% and 60%, respectively [28]. Dong et al. reported that IMT had a sensitivity and specificity of 53% and 77%, with a cutoff of 2.5 mm [29].
CEUS can quantitatively observe the newly formed nourishing blood vessels in the thickened vessel wall. Most studies have focused on CA assessment. Ma et al. found neovascularization in the wall of patients with active TAK to be located in the center of the wall [30]. The semiquantitative scoring employed in CEUS is: grade 0 (no angiogenesis, i.e., microbubble contrast agent is not found in the wall of the CA lesion); grade 1 (mild vascular formation, with a limited amount of mobile microbubble contrast agent observed in the wall of the CA lesion); grade 2 (moderate vascular formation, with a moderate amount of mobile microbubble contrast agent observed in the wall of the CA lesion); grade 3 (severe vascular formation, i.e., extensive vascular-wall formation, with clearly visible microbubble contrast agent). A CEUS semiquantitative score of ≥ 2 is used as the standard for active inflammation of the vessel wall. One meta-analysis showed that, using the Kerr score or PGA as the gold standard, the sensitivity and specificity of the CEUS semiquantitative score in diagnosing CA activity were 84% and 79%, respectively [17, 18, 29, 31]. The sensitivity and specificity of the CEUS semiquantitative score ≥ 2 were 95.5% and 69.2% [18], respectively, whereas the sensitivity and specificity of a CEUS semiquantitative score ≥ 3 were 59.5% and 96.1%, respectively [29, 31]. Two studies used PET/CT visual scoring as the gold standard. Authors found that the sensitivity of CEUS for diagnosing CA activity was 100%, and the specificity were 80% and 80.4%, respectively [32, 33], indicating that the diagnostic efficiency was comparable with that of PET/CT.
Diagnosis of TAK by MRAClinical question 8: Diagnosis of TAK by MRARecommendation 8: The diagnostic efficiency of MRA is comparable with that of DSA. MRA can be an effective alternative imaging modality to DSA. In patients who cannot use contrast agents, MRI can also clearly display aortic lesions (2 B).
Using DSA as the gold standard, Yamada et al. found that MRA had a diagnostic sensitivity and specificity of 100% for 20 patients with confirmed TAK and 10 patients with suspected TAK [34]. The sensitivity and specificity of three-dimensional contrast-enhanced magnetic resonance angiography (3D-CEMRA) for detecting stenosis and occluded lesions were 93.58% and 87.80%, respectively [35]. The sensitivity and specificity of 3D-CEMRA for detecting obvious stenosis lesions (> 50%) were 98.33% and 97.25%, respectively. Without the use of contrast agents, MRI can also be employed to describe systemic vascular lesions (including those in pulmonary arteries) in large-vessel vasculitis, making it a diagnostic method for patients who cannot tolerate contrast agents [36].
Clinical question 9: Evaluation of inflammation in the vessel wall by MRARecommendation 9: Thickening, edema, and wall enhancement around the circumference of the vessel on MRA are manifestations of active inflammation of the vessel wall (2 B).
Through short-tau inversion recovery (STIR), T2-weighted imaging (T2MI) and diffusion-weighted imaging (DWI) of MRA, edema and delayed enhancement of the arterial wall can be observed in active TAK [36,37,, 39]. Using Indian Takayasu Clinical Activity Score (ITAS) as the gold standard, two studies found that the sensitivity and specificity of wall thickening with enhancement in the diagnosis of disease activity were 66.7–100% and 85.7–89%, respectively [40, 41]. Zhang et al. reported the sensitivity and specificity of diagnosing disease activity through wall edema to be 66.7% and 84%, respectively [42].
Diagnosis of TAK using CTAClinical question 10: Diagnosis of TAK by CTARecommendation 10: CTA has diagnostic efficiency comparable with that of DSA. CTA can serve as an effective alternative imaging modality to DSA (2 B).
CTA can apply post-processing methods such as maximum intensity projection, curved projection reconstruction, and volume rendering to assist in displaying lesions in the wall and lumen of blood vessels. One small study included 25 patients with suspected TAK [43]. In that study, DSA was used as the gold standard for diagnosing TAK, and the sensitivity and specificity of diagnosing TAK by luminal lesions displayed by CTA were 95% and 100%, respectively. The sensitivity and specificity of diagnosing TAK with the lumen and wall lesions displayed by CTA were both 100%.
Clinical question 11: Evaluation of vessel-wall inflammation by CTARecommendation 11: Thickening and enhancement of the vessel wall in the arterial phase, and concentric low-density rings surrounding the vessel on the delayed phase of CTA, indicate active lesions (2 B).
One study evaluated 140 patients indicated that the sensitivity and specificity of assessing disease activity by using a maximum wall thickness of 3.3 mm on CTA were 83.1% and 89.7%, respectively, using the Kerr score as the gold standard [44]. A meta-analysis using the Kerr score or PGA as the gold standard showed that the sensitivity and specificity of CTA in diagnosing disease activity were 65% and 97%, respectively [43,44,, 46].
Diagnosis of TAK using PET/CTClinical question 12: Diagnosis of TAK by PET/CTRecommendation 12: PET/CT is not the preferred diagnostic method. If the nature of vascular lesions is unclear, or if an increase in the 18F- FDG uptake of the vessel wall is detected before morphological changes occur, it has certain value for the early diagnosis of TAK (4 C).
There is no direct evidence for using PET/CT in the diagnosis of TAK. The increased 18F- FDG uptake of the vessel wall on PET/CT is of reference value for the diagnosis of TAK. Several other diseases, such as inflammation of non-TAK and an unstable plaque in atherosclerotic regions, can also have an increased [19 ]F-FDG uptake, and which may be misdiagnosed as TAK. These diseases should be differentiated in clinical practice [47].
Clinical question 13: Evaluation of disease activity by PET/CTRecommendation 13: PET/CT can use semiquantitative methods to evaluate vascular inflammation. The PET Vascular Activity Score (PETVAS) can reflect systemic vascular inflammation and serve as a reference index for predicting recurrence and for monitoring the treatment response (2 B).
The visual scoring method for PET/CT is: grade 0 (no uptake); grade 1 (intake lower than liver intake); grade 2 (ingestion equals that of the liver); grade 3 (higher intake than that in the liver). Grades 2 and 3 are considered significant manifestations of vascular uptake of 18F-FDG. Based on vascular uptake of 18F-FDG, the literature proposes different indicators, such as SUVmax, SUVmean, and target-to-background ratio. According to different research reports, the cutoff of SUVmax for diagnosing TAK activity is 1.3–2.3, with sensitivity and specificity of 62.1–92.7% and 50–100%, respectively, using the Kerr score or PGA as the gold standard [19, 20, 46,47,48,49,, 51]. Two meta-analyses showed that the pooled sensitivity and specificity of 18F-FDG PET/CT for detecting TAK activity were 81% and 83%, respectively [52, 53]. These indicators arise from 18F-FDG uptake in a few lesion areas, and cannot reflect systemic inflammatory status or be used to evaluate the response to treatment. In 2018, Grayson et al. proposed PETVAS [54]. Based on 18F-FDG uptake, nine arterial regions (ascending aorta, aortic arch, descending thoracic aorta, abdominal aorta, right CA artery, left CA, brachiocephalic trunk, right subclavian artery, and left subclavian artery) were scored with visual scores ranging from 0 points to 3 points for each vessel, resulting in a total score of 0–27 points. In recent studies, PETVAS with a cutoff between 5.5 and 8 has been used to diagnose active TAK with a sensitivity range from 50 to 76.5%, and specificity range from 75.9 to 100%, using the Kerr score or PGA as the gold standard [50, 51, 55, 56].
The value of PET/CT in diagnosing TAK activity during immunosuppressive therapy is controversial. Grayson et al. found that ~ 60% of patients with clinically inactive TAK showed active signs of TAK upon PET/CT, which indicated subclinical vasculitis [54]. However, there is a lack of long-term follow-up data for vessels with signs of active TAK on PET/CT. Due to the unclear clinical importance of persistent imaging abnormalities, routine PET/CT examination is not recommended during the stable phase of TAK [17,18,19,, 21,
Comments (0)