FM patients, regardless of concomitant IMRD diagnosis, exhibit remarkably similar clinical characteristics. This is of interest, as the term ‘secondary FM’ is frequently used in IMRD patients, implying a potentially distinct pathophysiological mechanism of widespread pain, symptom severity or mental status. However, our results indicate a largely overlapping clinical profile in both groups, supporting the concept of a single disease entity characterized by central hypersensitization, sleep impairment and psychiatric comorbidities. A second key finding is that, despite generally lower FiRST scores in patients with IMRD, the evaluation of FM using the ACR2010 or FiRST criteria revealed comparable patterns across most clinical aspects. This supports the use of FiRST as a screening tool for FM in IMRD patients due to its simplicity. Moreover, FiRST places less emphasis on diffuse pain than the ACR2010 criteria and instead focuses more on central hypersensitization which may reduce interference from inflammatory rheumatic pain affecting joints or entheses. Finally, whilst enthesiopathy was significantly more prevalent in patients with concomitant IMRD in this study, it was less common in the FiRST cohort compared to the ACR2010 cohort.
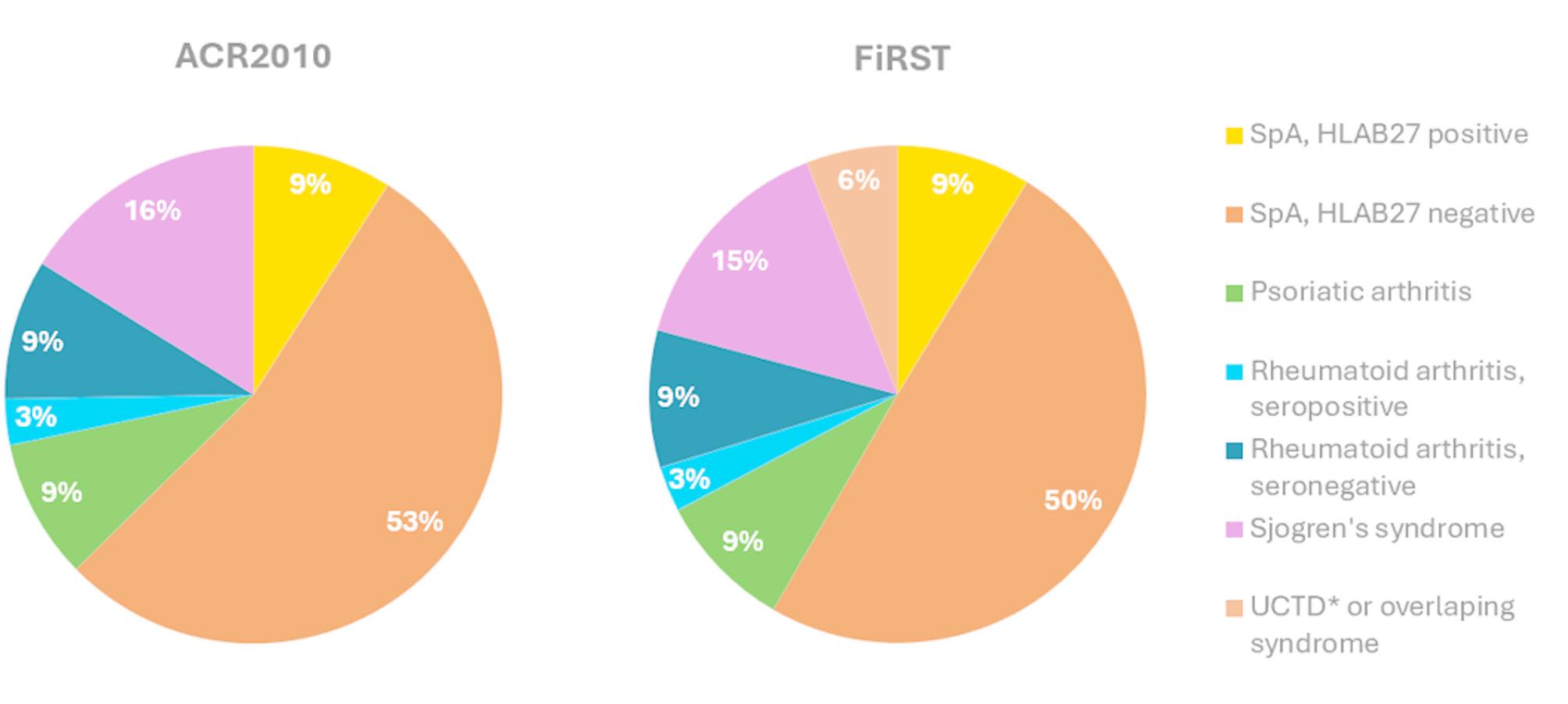
The most prevalent IMRD diagnosis in this cohort was HLA-B27-negative SpA, which may explain the higher prevalence of enthesopathy observed. This is particularly relevant for female patients with HLA-B27-negative SpA, as they have been reported to exhibit higher rates of enthesitis, to be less frequently HLA-B27 positive, and respond less effectively to immunosuppressants [20]. In the literature, the prevalence of FM SpA patient is notably high, ranging from 15 to 20% [15, 21].
In this cohort, alexithymia (emotional blindness) rates according to the TAS-20 questionnaire were notably high, affecting 64% of the IMRD group, and 60% of the non-IMRD group. In the literature, alexithymia was reported to affect 30% of SpA patients [22]. The most prevalent pain type in IMRD patients in our cohort was nociplastic rather than inflammatory, affecting both axial and peripheral regions. Notably, residual inflammatory disease activity was detected only in three patients. Nociceptive pain rates did not significant differ between the two groups, which may argue against the hypothesis that FM in IMRD patients is driven by an ongoing nociceptive or inflammatory stimulus. However, it is possible, that such stimuli initially triggered FM in susceptible individuals leading to persistent FM symptoms even after the stimuli ceased.
Despite the low sample size, an important limitation of this study is the reliability of the IMRD diagnoses, which were made prior to the study, often after several years of disease progression and multiple-line treatment failures. Nevertheless, disease activity was thoroughly assessed by clinical evaluations, laboratory analyses, and ultrasound examinations conducted both before and during the program. Another limitation is patient selection bias, as we only included patients participating in a tertiary, university-based, chronic pain multimodal pain program. This resulted in an exceptionally high prevalence of depression in both groups, ranging from 70 to 80%, far exceeding the 25% prevalence reported in the literature [23]. Nearly half of the patients in both groups were undergoing disability insurance process. Additionally, FM severity in this cohort is likely higher than in general clinical practice, as reflected by the high median Widespread Pain Index (WPI) score of 13 and Symptom Severity Score (SSS) of 9 in both groups. Two findings warrant further discussion: The higher incidence of childhood pain among FM patients with IMRD, observed in both the ACR2010 and FiRST groups, remains unclear, as no immunological explanation currently supports this association. FM patients with IMRD showed a more favorable response to the multimodal treatment program, particularly in the FiRST cohort. Apart from lower FiRST scores, IMRD patients responded better to intensive physiotherapy, which may be related to the higher prevalence of enthesopathy in this group. As FiRST also assesses whether physical activity worsens pain and fatigue, IMRD patients with lower FiRST scores may have benefited more from the multimodal program. However, the functional assessment at three months no longer showed a difference.
To our knowledge, this is the first study comparing MMP response in patients with an inflammatory rheumatic disease and concomitant fibromyalgia. However, the generalizability of our findings is uncertain due to significant heterogeneity in multimodal programs, including differences in duration in content [24]. Meanwhile, the FiRST criteria appear to be a simple and valid tool for detecting fibromyalgia in IMRD patients.



Comments (0)