
Remember me

She was seen at 9 months, following referral from National Eye Centre, for bilateral cataract, suspected congenital heart disease and poor growth from birth. The mother had history of transient rash in first trimester. She had several investigations done with a multidisciplinary team management for congenital rubella syndrome. Echocardiography revealed a PDA, but TORCHES screen was negative. At the age of 1, she had an eye surgery for bilateral cataracts and a PDA ligation at 18 months. Follow-up echocardiography done 4-year post-surgery showed thickened aortic valve with stiffness, regurgitation and bulging aortic root. SD was lost to follow-up for 7 years before re-presenting at 12 years, with 1 month history of body swelling and cough with difficulty in breathing of 1 week. She also had history of mental retardation, aphasia and poor sight and was not enrolled in any school.
Examination revealed a small for age child, in marked respiratory distress with nystagmus, restlessness, orthopnea, tender hepatomegaly, tachycardia, bi-basal fine crepitations, small volume radial pulse, elevated JVP, displaced apex beat, grade 3/4 diastolic murmur at aortic area and apical grade 3/6 systolic murmur radiating to the axilla. She received in-patient care for congestive cardiac failure. Echocardiography showed severe aortic stenosis and regurgitation, obstructive sub-aortic membrane, moderate mitral regurgitation and severe left ventricular dysfunction with an ejection fraction of 27%. Her diagnosis was based on WHO case definition for CRS as she had bilateral congenital cataract, a PDA, progressive aortic valve disease (severe regurgitation and stenosis) and mental retardation. See Figs. 1, 2, 3, and 4 below.
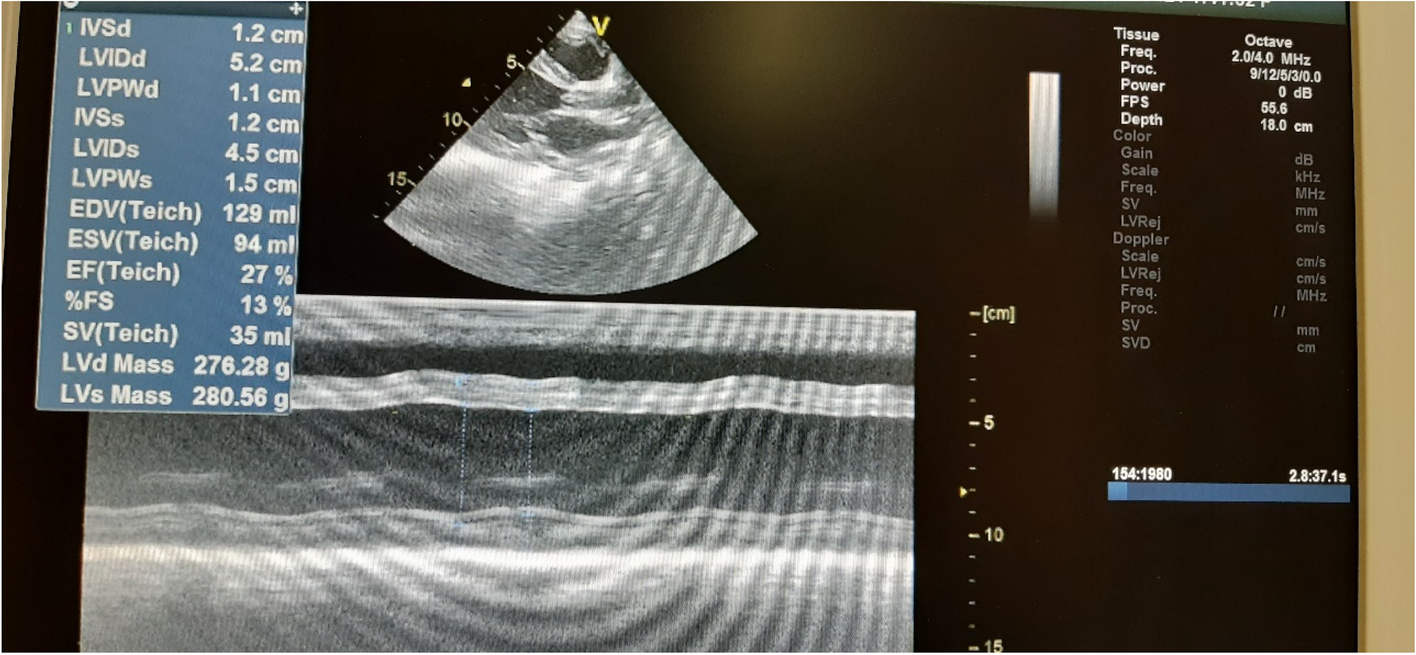
Fig. 1
Case 1: Severe LV dysfunction, EF = 27%, FS = 13%
Fig. 2
Case 1: Severe aortic stenosis in 2D, AV annulus = 12 mm (− 2.91 z), sinus = 15 mm (− 4.64 z), and ST junction = 13 mm (− 3.99 z)
Fig. 3
Case 1: Severe aortic stenosis, with AV mean PG of 51 mmHg
Fig. 4
Case 1: Severe AR, mean PG of 48.74 mmHg, and PHT of 104 ms
Case 2A 4-year-old female first seen at the National Eye Centre and National Ear Care Centre Kaduna with history of delayed developmental milestones, impaired hearing and whitish spot in left eye since birth. She was assessed by ENT specialist with the findings of congenital deafness and offered the option of bilateral cochlear implant. Parents brought the child to National Hospital for a second opinion. There was history of first trimester maternal rash.
Examination revealed a small for age child (weight at the 5th centile) with left eye cataract and horizontal nystagmus. TORCHES screening was IgG positive for rubella and Cytomegalovirus respectively. Echocardiography revealed a structurally normal heart. Ophthalmology review revealed salt and pepper retina and subcapsular pigments in the right eye and central lens opacity in the left eye. Though a rising IgG titre to rubella was not demonstrated because only one test was done, she was classified as clinically compatible CRS as she had two signs in WHO group A signs (hearing impairment and cataract).
Case 3The baby was admitted at 20 min of life on account of respiratory distress, sudden cyanosis, cardiac arrest and corneal opacity. She was a product of in vitro fertilization with a maternal history of transient rash in first trimester. Echocardiography showed a small-to-moderate PDA, mild pulmonary hypertension and trivial pericardial effusion. Maternal and patient’s TORCHES screening were both positive for rubella IgG and herpes simplex IgG. Ophthalmological review revealed microphthalmia and bilateral congenital glaucoma. She was managed for CRS and discharged subsequently and was on follow-up with the opthalmologist, paediatric cardiologist and paediatric neurologist before she was lost to follow-up. Though she was lost to follow-up and for a repeat TORCHES screening to monitor the IgG, she met the criteria for WHO clinically compatible CRS as she had a PDA and congenital glaucoma. See Fig. 5 below.
Fig. 5
Case 3: Microphthalmia and bilateral congenital glaucoma
Case 4The baby was admitted at 4 months and managed for severe sepsis with heart failure and suspected CRS. She had history of a small right eye with whitish speck and occasional rapid horizontal movements of the pupil. There was maternal history of febrile illness in first trimester, however, no rash. She was ill-looking with microphthalmia of the right eye and lenticular opacity, pale, febrile, tachycardic and tachypnoiec and had tender hepatomegaly, bilateral lung crepitations and grade 3 systolic murmur. Echocardiography revealed valvular and supravalvular mild-to-moderate pulmonary stenosis with smallish pulmonary artery and branches. Chest x-ray revealed cardiomegaly. TORCHES was negative. Ophthalmology review noted microphthalmia, fine amplitude pendular nystagmus with unilateral right cataract. She was referred for further ophthalmological management and to continue follow-up with the paediatric cardiologist. Although the TORCHES screening was negative, she met the criteria for clinically compatible CRS as she had congenital cataract and valvar and peripheral pulmonary stenosis. See Figs. 6, 7, 8, and 9 below.
Fig. 6
Case 4: Lenticular opacity of the right eye
Fig. 7
Case 4: Smallish main pulmonary artery (7 mm)
Fig. 8
Case 4: Smallish left pulmonary artery (6 mm)
Fig. 9
Case 4: Pulmonary valve stenosis with peak gradient of 42 mmHg
Comments (0)