This single arm clinical trial was conducted on 40 pediatric patients with partial rectal prolapse not responding to common conservative measurements at Cairo University Specialized Pediatric Hospital.
The main idea of the study is to combine two minimally invasive approaches commonly used for treatment of partial rectal prolapse in children to increase the success rate of the combined approach more than the classic single approach.
We believed that recurrence of rectal prolapse after injection sclerotherapy is mainly due to early postoperative straining for defecation that would not give enough time for the sclerosants agent to exert its intended fibrosis and rectal mucosal fixation.
Also the recurrence post anal cerclage may occur due to single plane of mucosal fixation as the circular suture taken in one line that can’t stand long against the repeated straining and the weight of a heavy loaded rectum.
We decided to combine both approaches to gain benefits of each one owing to decrease the failure rate to the least level as we believed that cerclage will fix the rectal mucosa in place for a while enough to buy suitable time for the injected sclerosant agent to exert its sclerosing effect.
We chose the hypertonic saline as a sclerosing agent as it is safe, easy to prepare, cheap, sterile and is the least harmful for the rectum and other pelvic structures if injected in a higher dose or extravasated.
Hypertonic saline initiates a chemical inflammatory reaction that results in fibrosis around the rectal wall and perirectal tissue that causes the mucosa to adhere to the rectal wall and the rectum to adhere to the perirectal tissue and so it prevents recurrence of prolapse. The post-operative recurrence among our patients was 5%, and they needed post-operative 2nd operation for recurrence. Only a few studies that have used 15% hypertonic saline are available at present for the management of rectal prolapse in children for comparison.
The recurrence rate in our study was lower than that reported by Chaudhry et al. as they detected that in the 5% phenol group, 24% (n = 12) and in hypertonic saline group 46% (n = 23) had recurrence of rectal prolapse [4]. Relatively similar to ours, Abes et al. and Mustafa et al. who also used 15% hypertonic saline for the management of rectal prolapse in children; they reported that only one patient from among 16 children required a second treatment after the first injection [1, 16]. In UK, Shah et al. carried out a study on 24 patients with persistent rectal prolapse. Children below the age of 5 years, group I (n = 17), were successfully managed by submucous hypertonic saline injections and only 17% had recurrence [19]. Injection therapy is usually the first-line treatment at a majority of centers. We believe that we had the least recurrence rate among other published studies because we do concomitant cerclage with injection sclerotherapy that exerts a mechanical fixation of the rectal mucosa for a suitable time enough to gain the proper effect of the injected sclerosant agent.
In the current study, the mean age of all studied patients was 5.53 ± 2.9 years with age range 2 −13 years. There were 24 males (60%) and 16 females (40%) in the studied patients. The mean weight of all studied patients was 24.8 ± 10.2 kg (12–52 kg). As regard family history of rectal prolapse, there were 4 patients (10%) with positive family history in the studied patients.
Likely, a randomized control trial that was conducted by Chaudhry et al. on 100 children with grade I or grade II rectal prolapse, reported that the mean age was 6.61 (± 2.75) years. The study included 55% (n = 55) males and 45% (n = 45) females [4]. Similarly, a prospective study included 24 pediatric patients diagnosed with rectal prolapse with age ranged from 2.5 to 14 years with average of 7 years old. There were 18 males and six females. Six patients had positive family history of rectal prolapse [7]. Also, a prospective study conducted by Sharma et al.on 107 pediatric patients with rectal prolapse, the average age was 4.2 years (range: 1–18 years). The male:female ratio was 8:3 [20].
As regard governmental distribution, The data provides valuable insights into the distribution of children with rectal prolapse across different governmental regions in Egypt. Fayoum Governorate had the highest rate of rectal prolapse cases in our study, and the possibility of this is due to a poor standard of living or being an agricultural environment and a high chance of parasitic infestation.
In the present study, the mean duration of disease was 14.4 ± 4.04 months (12 months – 30 months). Likely a study conducted by Kayastha et al. on 50 patients with idiopathic partial rectal prolapse, in whom conservative management failed, revealed that the mean duration of rectal prolapse was 11 + −6.9 months [12].
The clinical data among our patients, there were 23 patients (57.5%) with no need for manual reduction, 10 patients (25%) with some times need for manual reduction and 7 patients (17.5%) with manual reduction need in every motion. As regard parasitic infestation, there were 12 patients (30%) with parasitic infestation in the studied patients. Also, Gad et al.detected (42%) 10 of them prolapse was reduced spontaneously, (42%) 10 of them needed manual reduction after every prolapse and (16%) 4 sometimes needed manual reduction, also that 11 (45%) patients had history of parasitic infestation which was treated preoperatively [7].
Constipation and parasitic diarrhea are the main contributing factors in children [9]. Among our patients, the mean preoperative constipation score of all studied patients was 9.55 ± 7.06 with minimum score of 0 and maximum score of 22. A cross-sectional study included 29 children with prolapse, detected that four children had a normal transit with at least one bowel movement a day, compared with 19 cases of chronic constipation and 6 cases of diarrhea [15].
The mean surgical duration in our studied patients was 9.2 ± 1.04 min with minimum duration of 7 min and maximum duration of 11 min.
The mean surgical duration of 9.2 min is relatively short, which is consistent with other studies. A study published in the Journal of Pediatric Surgery found that the mean surgical duration for hypertonic saline injection was 7.4 min (± 2.1 min) [13]. Another study published in the Journal of Pediatric surgery reported a mean surgical duration of 8.5 min (± 1.5 min) [22].
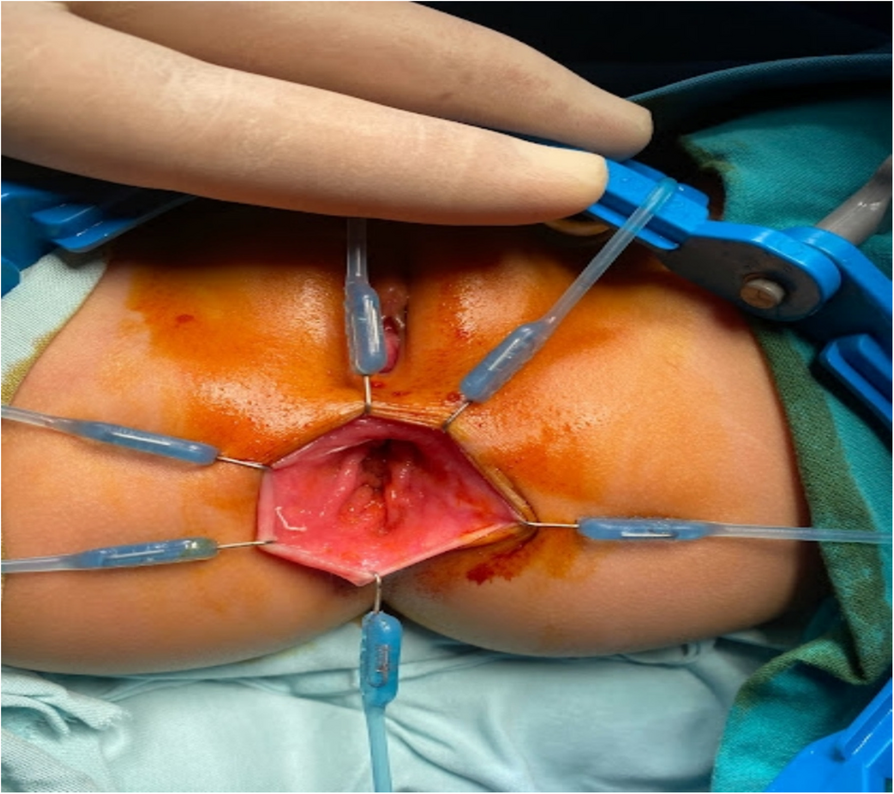
We found that the operative time is not very long and consistent with other published studies however we do a combined injection – cerclage approach. We believe that using the Lone Star retractor is very helpful to shorten the operative time as it helps proper exposure and demarcation of the landmarks and makes the injection very secure and under vision. Also the cerclage is easier by the guidance of the suitable Hegar dilator.
The description of post-operative complications in all studied patients, there were 7 patients (17.5%) with post-operative bleeding, 1 patient (2.5%) with post-operative diarrhea, 6 patients (15%) with post-operative constipation, 7 patients (17.5%) with post-operative fever and 2 patients (5%) with post-operative rectal inflammation, both patients were treated medically without the need for surgical evacuation or diverting colostomy. When we searched for the possible cause of this incident the only factor that may be involved that both patients had some sort of infective diarrhea few days before the development of this localized rectal inflammation. Kayastha et al. detected that only one patient (2%) had perianal abscess which was drained successfully [12]. Chaudhry et al. reported that in hypertonic saline group 2% (n = 1) had postoperative fecal incontinence and 2% (n = 1) had anal stenosis [4].
Several factors contribute to the high reduction of pain that was present preoperatively:
Osmotic Effect: Hypertonic saline creates an osmotic gradient that leads to the absorption of water from the prolapsed tissues. This can reduce edema and congestion, relieving pain and discomfort associated with the prolapse.
Sclerosing Action: The saline solution induces a mild inflammatory reaction in the tissues, leading to fibrosis. This fibrosis can fix the rectal tissues in place, preventing further prolapse and associated pain.
Reduction of Prolapse: By shrinking the prolapsed tissue through osmotic dehydration, the prolapse is reduced, decreasing the stretching and pressure on the anal sphincter and surrounding tissues that cause pain.
Nerve Desensitization: Hypertonic saline can have a desensitizing effect on local nerve endings, decreasing post operative pain perception in the affected area. Minimal Invasiveness: Compared to surgical interventions, hypertonic saline injection and cerclage are minimally invasive, reducing the trauma and pain that can accompany more invasive treatments [14].
Study limitations
Some limitations also need to be addressed. Firstly, it was single center study, which, despite potentially limiting its external validity, provides consistency. Additionally, the sample size in this study was relatively small. Finally, the lack of long-term follow-up.


Comments (0)