GTDC is an uncommon congenital entity (1:4500) with a slight male predominance. Commonest site for GTDC is the ileum (33%), followed by esophagus (20%), colon (13%), jejunum (10%), stomach (7%), and duodenum (5%) [4, 5]. It can be divided into cystic or tubular type [6]. The most common GTDC is spherical non-communicating cyst. Tubular GTDC is less common, which runs parallel to adjacent alimentary tract with communication to the normal bowel [7, 8]. GTDC can also be classified into parallel type (type I) and intramesenteric type (type II) based on the vascular supply to the bowels [9]. Extensive GTDC of the small bowel involving the intermesenteric region and retroperitoneum is exceedingly rare and has not been reported in the English literature.
Clinical presentation varies depending on the histopathology, type, location, and size of the duplication cyst. It can be an incidental finding during surgery for an unrelated condition [10]. The nonspecific nature of symptoms may mimic other gastrointestinal problems and cause delay in diagnosis. This patient presented with nausea, vomiting, epigastric pain, and failure to thrive which were initially treated as gastritis. Recurrent episodes of pain may be attributed to mucosal ulcers from gastric acid secretions and accumulation of secretions within the duplication cyst resulting in increased pressure [11]. Chronic anemia can be explained by chronic ulcers causing bleeding within the cyst. The combination of recurrent abdominal pain leading to poor oral intake and chronic ulcers with anemia was believed to be the cause of failure to thrive in this child. Other complications arising from bowel duplication include infection, gastrointestinal bleeding, and perforation due to the presence of ectopic gastric mucosa [12]. Ileal GTDC can be a lead point for intussusception or intestinal obstruction. Volvulus, torsion, or extrinsic compression to adjacent structures are other possible complications. Malignant transformation of the ileal GTDC, e.g., lymphangiosarcoma or sarcoma, has been reported [13].
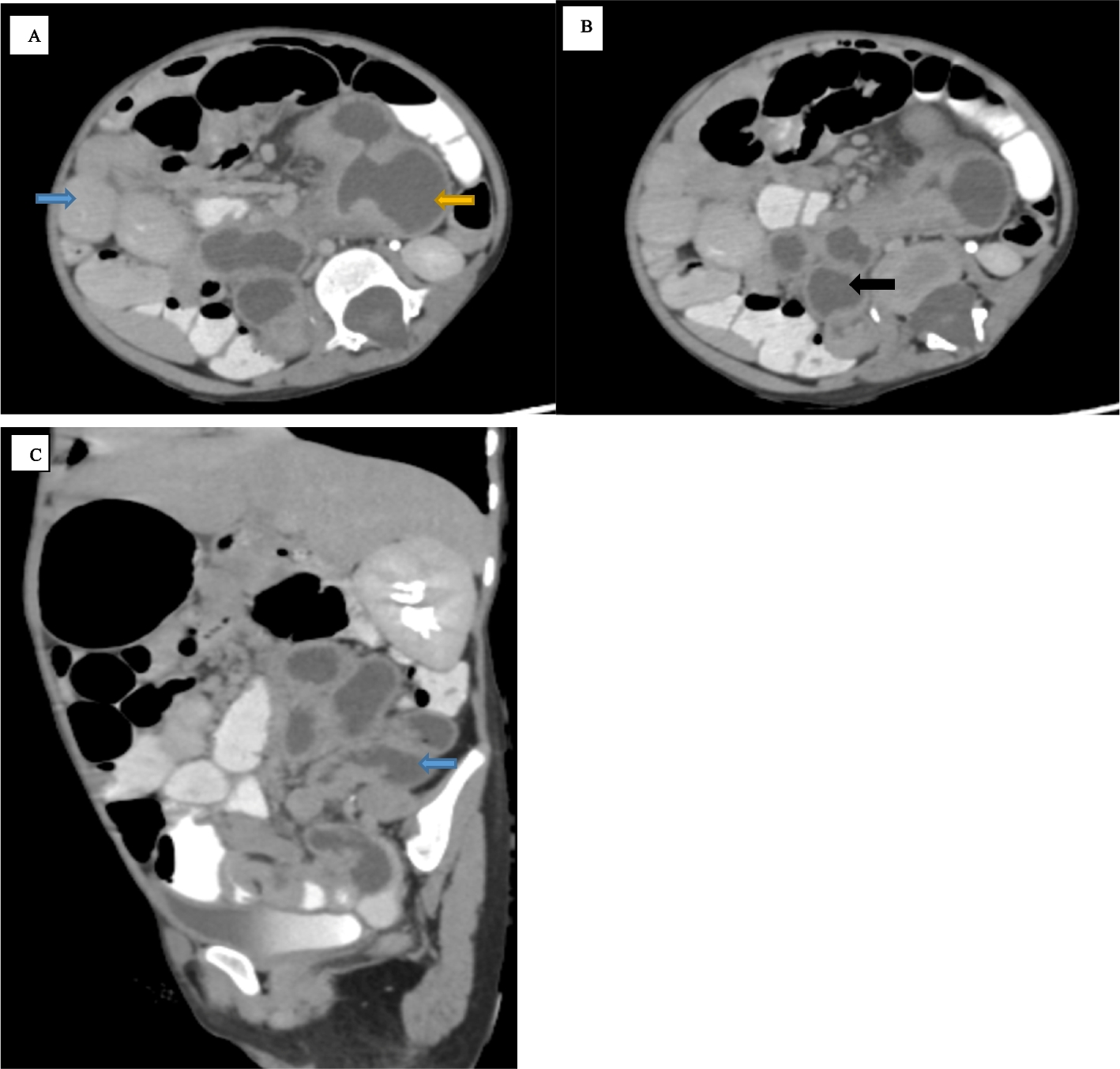
Antenatal scan may reveal an intra-abdominal anechoic lesion with or without double wall or gut signature sign [14]. Infrequently, ileal GTDC may present as an echogenic mass secondary to bleeding within the cyst. Polyhydramnios could be an antenatal ultrasound feature to support in utero bowel obstruction. Abdominal radiograph may show nonspecific features and is less helpful for diagnosis of GTDC. Ultrasound abdomen should be the first diagnostic modality. Ultrasound may show a cystic or tubular lesion with echogenic inner mucosa layer and hypoechoic outer muscular layer [14]. Other ultrasound features of GTDC include five-layered cyst wall and “Y” sonographic configuration [15]. However, identification of these aforementioned signs requires expertise and high-resolution ultrasound. Detection of the cyst may be missed if the cyst is collapsed. This maybe the reason that the cyst was not detected during the initial ultrasound for our patient. In situations where there is difficulty differentiating thickened bowels from a GTDC, CECT abdomen with oral and IV contrast is helpful in demonstrating the anatomical location of the cyst and its relationship to adjacent structures.
If diagnosis can be made by ultrasound, computed tomography should be avoided in the pediatric age group to reduce radiation. CECT will normally show a thin cystic or tubular structure adjacent to the small bowel loops with mild wall enhancement. Hyperattenuating material within these structures may represent hemorrhagic or proteinaceous products. Infected ileal GTDC may have CT features of air pockets within a thick enhancing wall with surrounding fat streakiness.
The small bowel follow-through may show displacement of the small bowel loops by the cyst and its communication with the adjacent bowel lumen [16]. Ectopic gastric mucosa can be detected by using TC-99 m pertechnetate scintigraphy [17]. This scintigraphy can help to differentiate ileal GTDC from Meckel’s diverticulum, which the latter is usually located at the anti-mesenteric border of the ileum and adjacent to the ileocecal valve [6].
Differential diagnosis for tubular type ileal GTDC includes Meckel’s diverticulum, lymphangioma, and pancreatic pseudocyst, which can be found adjacent to the mesentery or retroperitoneally. Omental cyst, mesenteric cyst, enteric cyst, pancreatic pseudocyst, and lymphangioma are differential diagnosis for cystic type of ileal GTDC.
Complete excision remains the main aim of surgical management. In situations where extensive bowel involvement is present, other methods to preserve bowel length can be used such as marsupialization, Wrenn’s procedure, and Soper’s procedure [17]. Wrenn’s procedure involves stripping of the mucosal layer of the duplicated bowel while preserving the seromuscular layer to avoid devascularizing the blood supply to the adjacent normal bowel. In cases for long colonic duplications, a connection is made at the distal blind end of the cyst with the normal bowel to decompress the stools (Soper’s procedure).


Comments (0)