Kidney diseases among children are considered as a huge health burden. Adequate documentation and knowledge of kidney disease load are important steps in preforming accurate registry that help in proper allocation of the resources [11].
We aimed to identify the clinical profile of pediatric patients attending nephrology outpatient clinic at Children’s Hospital Cairo University by collecting data of 365 children who attended the pediatric nephrology outpatient clinic over 6 months duration.
Male percentage in the present study was 64.4%. In line with our study, kidney diseases showed male predominance in patients with kidney disease [3, 12, 13]. Male predominance in the current study could be explained by the common diseases in our population which are more common in males. Nephrotic syndrome affected 122 patients and it might be more common in males than females [14]. Moreover, 111 patients had CAKUT; that are strongly correlated with male sex [15].
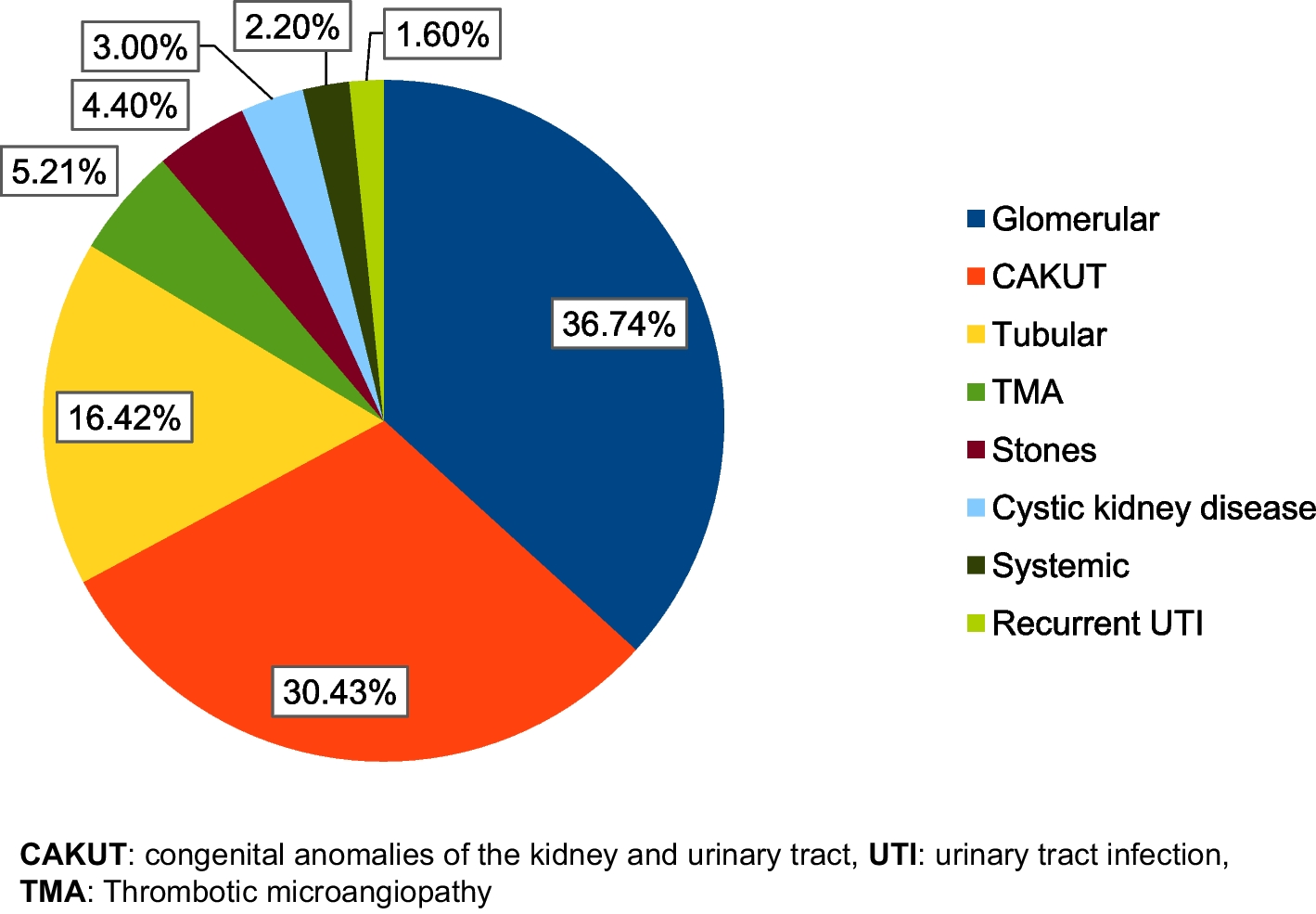
Regarding the etiology of kidney diseases among our studied patients, the most commonly reported etiologies were glomerular diseases that were present in 134 (36.7%) patients, followed by CAKUT that were affecting 111 (30.4%) patients.
Also, in another Egyptian study which included 142 patients admitted in hospital with kidney disease, glomerular diseases were the most common pediatric kidney disease including 62 (51.2%) patients followed by CAKUT (33 patients, 27.3%) [3].
While in contrast with our study, CAKUT were the commonest kidney diseases in 39% of children, followed by acute glomerulonephritis in 32.7% of patients in the study performed by Kansakar et al. (2021) on 352 children [12]. Furthermore, Mola and Shimelis (2016) revealed that the three most common kidney diseases observed were CAKUT seen in 26.8% of patients, followed by NS in 16.9% of patients and acute glomerulonephritis in 12.2% of patients [16]. The differences in the results of the previous studies confirm that the pattern of childhood kidney disease is variable and differs from one region to another [1].
In the present study, the most common disease among patients with CAKUT was PUV in 35 (31.5%) patients, followed by solitary kidney in 18 (16.2%) patients. The least common disease was meatal stenosis reported in 2 (1.8%) patients. In line with our study, PUV was the most common detected anomaly among CAKUT patients in another Egyptian study [17]. In disagreement with our results, most of the children with CAKUT in Kansakar et al. (2021) study had VUR [12]. Meanwhile, other studies found PUJ obstruction to be the commonest CAKUT [18].
The most common disease among patients with glomerular disorders in the present study was nephrotic syndrome in 122 (91%) patients. Meanwhile, Kansakar et al. (2021) study revealed that post-streptococcal glomerulonephritis was the commonest glomerular disease, followed by SLE nephritis [12]. Moreover, in Ahmad et al. (2019) study that included182 patients who had glomerular diseases, and the commonest glomerular disease was glomerulonephritis in 73 (40.10%) patients [17].
The most common type among patients with NS in the present study was SRNS in 87 (71.4%) patients with NS. In disagreement with our study, steroid sensitive NS in Kansakar et al. (2021) study was the most common type of NS followed by steroid dependent NS (SDNS) and SRNS [12]. Also, PriyadarShini and Pradhan. (2019) study on 443 children reported that SDNS was the most frequent among all NS children [13].
Out of 111 patients with CAKUT in the current study, 71 (63.9%) patients were diagnosed prenatal. In line with our study, 60% of CAKUT patients were diagnosed antenatal in Ahmad et al. (2019) study [17]. Moreover, intrauterine detection or suspicion of CAKUT occurred in about 65% of Radhakrishna et al. (2019) study population. Furthermore, they reported that third-trimester ultrasound was more accurate in detection of CAKUT antenatally. This shows the importance of antenatal ultrasound in diagnosis of CAKUT that help in proper timing for postnatal intervention [18].
Anemia was reported in 223 (61.1%) patients in the current study. Lower incidence of anemia was reported by Masalskienė et al. (2021) study that included 172 children, 19.6% of children had anemia [19]. Also, eGFR was significantly positively correlated with hemoglobin level. Similarly, Warady et al. (2015) in their study on children with kidney diseases, reported that the median hemoglobin decreased as the measured eGFR declined to < 43 ml/min/1.73m2 [20]. Anemia is a common morbidity in children with CKD. It is caused by inadequate erythropoiesis, iron deficiency, and inflammation. Furthermore, there is difference in individual hemoglobin levels at any given eGFR, and is affected by race and ethnicity factors. Most of these patients are receiving treatment with erythropoiesis-stimulating agents and iron therapy, but the incidence of anemia resistant to treatment is still high [21]. Low hemoglobin level and high erythropoietin dose are considered predictors of erythropoietin resistance [22].
Growth impairment is very common in children with CKD and may be the most noticed comorbidity in them. The children and infants and patients with advanced stages of CKD are especially affected by growth impairment [23, 24]. In the current study, 156 (42.7%) patients had growth impairment. CAKUT, renal tubular diseases and cystic kidney diseases are significantly associated with growth impairment. Growth impairment could be explained by the presence of metabolic acidosis that is commonly associated with resistance to growth hormone and stimulates calcium mobilization from bone. Also, multiple factors could restrict the growth as anorexia, poor caloric and protein intake, electrolyte, water and mineral losses [24].
In the present study, 29.6% of patients were underweight, 39.2% of patients were stunted. Higher prevalence of stunted growth and weight loss were reported by Radhakrishna et al. (2019), 59% of patients were underweight, 37% of patients were stunted [18].
Uncontrolled hypertension is a risk factor for CKD progression leading to cardiovascular comorbidity and is one of the commonest causes of death in pediatric patients with CKD [21]. Hypertension was reported in 175 (47.9%) patients in our study. Higher prevalence of hypertension was reported by Masalskienė et al. (2021) study; hypertension was diagnosed in 60% of children [19]. Lower prevalence of hypertension was reported by Radhakrishna et al. (2019) study on 81 patients with CAKUT; hypertension was found in 27% of cases. The differences can be attributed to inclusion of CAKUT patients only in Radhakrishna et al. [18].
Hypertension is a major risk factor of vascular stiffening affecting the kidney microcirculation. Endothelial injury and kidney with areas of hypoperfusion as kidney cysts, scaring or dysplastic tissue increase renin secretion leading to activation of renin–angiotensin–aldosterone [25].
Estimated GFR was significantly decreased in patients with SBP percentile > 99 when compared to patients with SBP percentile between 95 and 99 (P = 0.031), as well as patients with SBP percentile < 90 (P = 0.006). Also, eGFR was significantly decreased in patients with SBP percentile between 95 and 99 when compared to patients with SBP percentile < 90 (P = 0.016).
Hypertension is mainly related to the primary kidney disease rather than CKD stage. Glomerular kidney are more commonly associated this hypertension than CAKUT [26].
Patients with CAKUT had significantly higher incidence of anemia when compared to patients who didn’t have CAKUT (72.1% vs 56.3%; P = 0.004). Similarly, a study by Bizerea-Moga et al. (2019) that included 22 patients with CAKUT and 19 patients with glomerular disease, revealed that CAKUT often had associated anemia (27.3%) [27].
Patients with CAKUT had significantly higher incidence of growth impairment when compared to patients who didn’t have CAKUT. In agreement with our finding, other studies reported that pediatric patients with CAKUT have higher incidence of growth impairment than patients with glomerulonephritis [28, 29]. Children suffer from CAKUT have high incidence or recurrent UTI. Kidney insufficiency is a well-known complication, either from pyelonephritis, a preexisting congenital kidney anomaly which predisposes the child to UTI, or from the use of nephrotoxic antibiotics. Electrolyte and acid–base disturbance may be present [30]. In the present study, metabolic acidosis was reported in 149 (40.8%) patients.
Patients with glomerular kidney diseases had significantly lower incidence of growth impairment when compared to patients who didn’t have glomerular kidney diseases. In agreement with the current study, another study conducted by Rodig et al. (2014) reported that pediatric patients with CKD due to glomerular diseases had significantly higher height SD compared to pediatric patients with CKD due to non-glomerular diseases [31].
Glomerular filtration rate had positive significant correlation with height Z score (r = 0.367; P < 0.001). In line with our study, growth rate and GFR were found to decline in parallel; Rodig et al. (2014) detected a decline in height SD score of 0.12 to 0.16 for each decrease of 10 ml/min/1.73 m2 [31]. Moreover, Furth et al. (2011) reported that there was a three-fold higher risk of growth impairment in pediatric patients with CKD with eGFR < 30 ml/min per 1.73 m2 when compared with others having eGFR ≥ 50 ml/min per 1.73 m2 [32].


Comments (0)