We used a combination of surgeon’s X-ray assessment and OSTA to predict osteoporosis in Japanese women who underwent hip surgery. In the analysis, the surgeons’ assessment had “moderate” to “good” predictive ability, whereas the OSTA score had “good” predictive ability. When both scores were combined, the AUCs were “good” in 11 surgeons and “excellent” in four surgeons. Collectively, our results indicate that combining surgeons’ assessment and OSTA can be used as a simple convenient screening tool for osteoporosis that can help identify patients who may need further BMD assessment using DXA.
Comparison of our results with those of previous reports
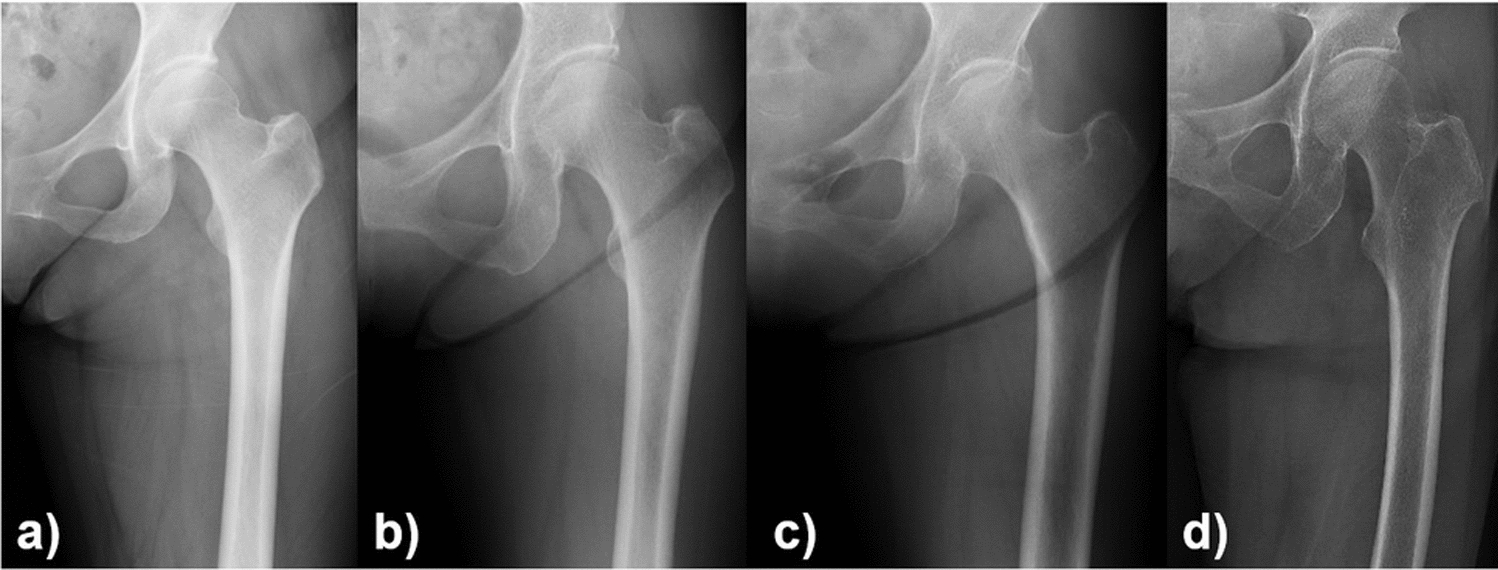
The effectiveness of using hip X-ray findings in screening for osteoporosis has been reported. For example, the usefulness of parameters, including the Singh index, cortical thickness index, canal flare index, canal-to-calcar ratio, and Dorr classification, has been analyzed. Among them, several studies have reported the usefulness and superiority of the cortical thickness index with an AUC of 0.82–0.84 for diagnosing osteoporosis [12, 27, 28]. In the present study, the AUC from X-ray assessment ranged from 0.626 to 0.875 across surgeons, and the AUC using the ave.pred-score was 0.890, indicating that surgeons’ assessment had high predictive ability to detect osteoporosis from hip X-rays. Conversely, the causality of each surgeon in selecting the pred-score remains unknown and is subjective. However, surgeons likely define their pred-score based on X-ray findings (e.g., cortical thickness and bone structure of the cancellous bone). Although subjective, the intraobserver agreement of the pred-score was “almost perfect,” and no significant difference was found between staff surgeons and residents. Thus, the results support the application of the pred-score in clinical practice regardless of the surgeon’s experience.
With regard to OSTA, previous studies have demonstrated its effectiveness as a screening tool for osteoporosis. Specifically, previous studies have reported that the OSTA has an AUC value ranging between 0.62 and 0.87 [18,19,20,21,22]. In the present study, the AUC of the OSTA score was 0.817, which was included in the range reported previously.
Some studies have reported the usefulness of combining X-ray findings and OSTA. For example, Liu et al. [29] reported that combining the Singh index and OSTA significantly improved the AUC for diagnosing osteoporosis (0.795) compared with using the OSTA (0.534) or Singh index (0.636) alone. While a direct comparison with our study could not be made, the results of our study were likely superior to those of Liu et al’s study, as previous studies have shown the difficulty of using the Singh index in predicting the BMD of the proximal femur.
Application of the results to clinical practice
In this study, the AUC (0.912) combining the ave.pred-score and OSTA score was significantly improved compared with that of the OSTA score (AUC: 0.817) when analyzed in all surgeons. Alternatively, no significant improvement of AUC was found from the ave.pred-score. When analyzed for each surgeon, the AUC was the highest when the pred-score and OSTA score were combined, with significant improvement from AUCs calculated with the pred-score or OSTA score in 11 surgeons (73.3%). Because X-ray assessment is usually performed by surgeons in their clinical practice (e.g., outpatient clinic), our results support its clinical application regardless of the surgeon’s skill in predicting osteoporosis from hip X-rays. As the method proposed in the present study is not applicable for assessing BMD changes over time, our next step is to clarify factors that enable longitudinal BMD assessment.
There may be other methods to further improve the prediction of osteoporosis screening, including adding other metrics calculated from X-rays (e.g., Singh index, cortical thickness index). However, the addition of several parameters requires time and increases the complexity in measurement and analysis, limiting its use in clinical practice. As “good” or “excellent” AUCs (>0.82) were maintained among all surgeons, we believe that the method developed in this study is clinically useful for osteoporosis screening in patients with hip diseases.
The recent application of artificial intelligence (AI) technology for screening osteoporosis from hip X-rays has considerable attention. In fact, some studies have shown an AUC of >0.9 in detecting osteoporosis from hip X-rays [30,31,32]. While the “black-box” aspect of AI is a matter of concern, our results may explain why adding patient demographics to the AI model improved the predictive accuracy of osteoporosis [30]. As our study has shown that combining the ave.pre-score and OSTA score maintained an AUC of >0.9, we believe that it would be necessary for future studies to compare the results derived from AI and those derived from other conventional methods in order to clarify the novelty and usefulness of a new AI system.
Application of the results to patients from other countries and males
Although the OSTA was originally developed for postmenopausal Asian women, studies have confirmed its potential use in osteoporosis screening for men and other ethnicities, including Caucasians and African-Americans [33]. For example, previous studies have reported an AUC of 0.71 for men (94% Caucasians) [34], an AUC of 0.813 for Caucasian women [35], and a sensitivity of 75.4% and specificity of 75.0% with a cut-off value of 2 for African-American women [36]. Thus, while further studies are necessary, we believe that there is a potential for the findings of this study to be tested and validated in different cohorts.
Limitations
This study has some limitations. First, as information regarding menopause was not available, the patients included in this study were women aged over 40 years. The results may vary if only postmenopausal women were included. Second, the results may not be directly applied to the general population, as the patients analyzed in this study were scheduled for hip surgery due to hip disorders. Although a study acquiring hip X-rays in a healthy population could be conducted, the radiation dose cannot be ignored. As hip X-rays are routinely acquired preoperatively and postoperatively for patients with hip diseases, we believe that the lack of analysis in the general population does not diminish this study’s clinical importance. Third, while hip X-rays were acquired following routine protocol with the lower limb internally rotated, the femur was not always in the neutral position because of its anatomy or disease in the contralateral hip. Our next step may be to clarify the effect of hip rotation on the pred-score of each surgeon because hip rotation may alter the surgeon’s assessment of the femur.
Conclusions
Surgeon’s X-ray assessment and OSTA had the potential to be used for osteoporosis screening. When the ave.pred-score and OSTA score were combined, the AUC to detect osteoporosis was 0.912. When analyzed for each surgeon, an AUC > 0.82 was maintained across surgeons regardless of their experience when the pred-score and OSTA score were combined. Collectively, our results confirmed that combining the surgeon’s hip X-ray assessment and OSTA is a potentially useful tool to easily screen for osteoporosis and help identify patients who require DXA examination.






Comments (0)