Mechanism and clinical manifestations of sacral TCs
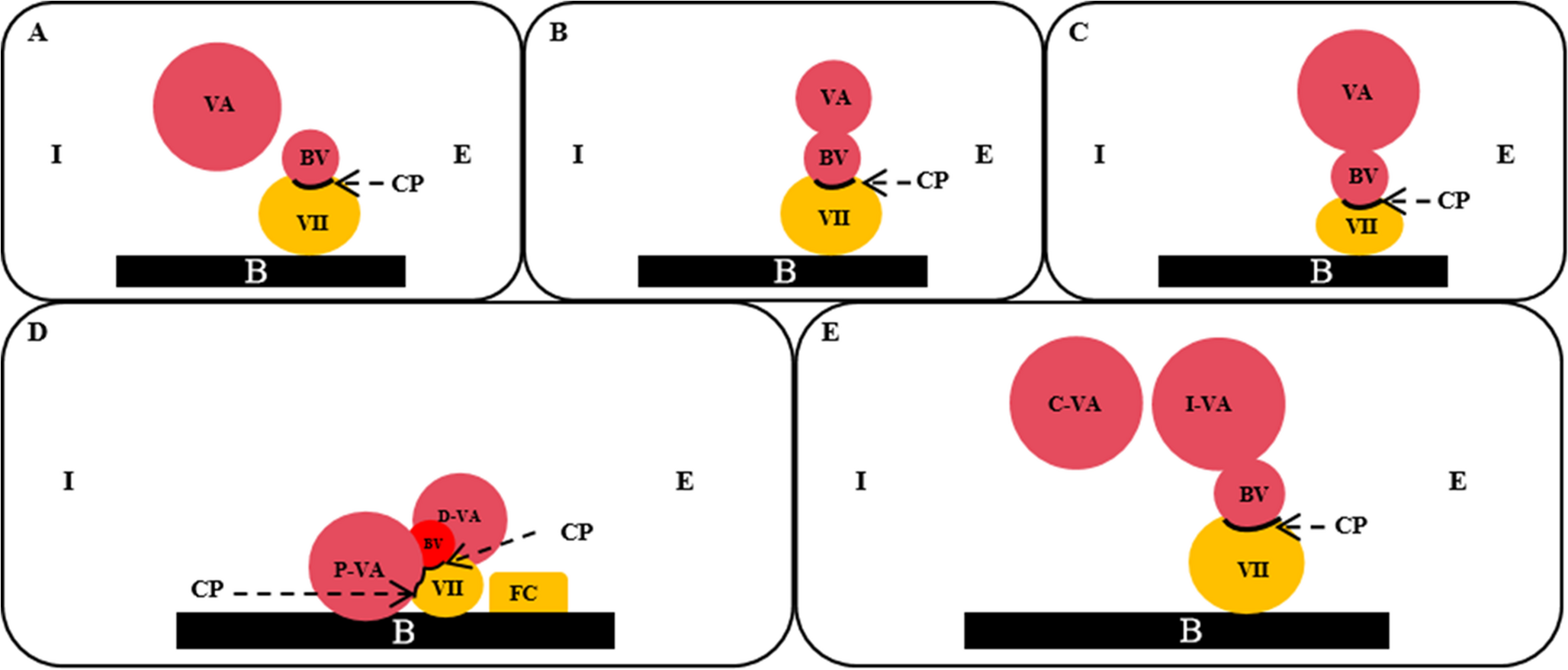
Most scholars recognize the ‘ball-valve mechanism’ theory regarding the formation of TCs. Due to congenital disorders (e.g., Ehlers-Danlos syndrome [9], Marfan syndrome [10], etc.) or acquired factors (including trauma, inflammation, etc.), when local hydrostatic pressure rises, cerebrospinal fluid flows unidirectionally through the potential space between the nerve tract membrane and the endurum, gradually expanding and resulting in cyst formation [11].
The mechanism of these symptoms usually involves nerve tension and torsion from cerebrospinal fluid-induced shear force and tension from the cyst wall on the nerve root. Clinically, many single cysts’ symptom areas exceed the innervation area of their carrying nerve, meaning cysts can compress surrounding roots and cause symptoms. Thus, surgeons should remove the cyst-occupying effect for better symptom relief.
The surgical approach plays a crucial role in determining the prognosis following the surgical treatment of spinal arachnoid cysts. One study showed that cyst excision is very effective for spinal arachnoid cysts with an extremely low complication rate [12]. In this study, we concluded that the postoperative recurrence of sacral TCs might be associated with the initial surgical methods, such as puncture aspiration, laminectomy, and shunt, which fail to appropriately manage the fistula of sacral TCs. Additionally, if the wall of the residual cysts is extremely thin, the reconstructed nerve root sleeve might be incomplete, and its tension may be inadequate to counteract the hydrostatic pressure. Consequently, this study suggests that resolving the fistula problem and ensuring sufficient tension of the reconstructed neurogenic sleeve are essential for effectively addressing the issue of postoperative recurrence of sacral TCs.
Multiple dimensions of radiographic reconstruction
For postoperative recurrent sacral TCs, the situation is highly complex after the initial surgery. Before secondary surgery, using imaging to determine the cyst’s location, leakage source, nerve presence and origin within the cyst is crucial for prognosis.
The clinical application value of MRI 3D-FESTA technology is widely recognized in medicine. The enhanced 3D-FIESTA-C sequence, considering the sacral canal’s anatomy, improves the contrast issue in traditional T2 or T1 sequences. Nerve roots in sacral TCs have low signal intensities, contrasting with the high CSF signal in the cysts.
3D images reconstructed spherically in any dimension can display the anatomical relationship between the nerve root and sacral TCs from various angles. Based on 3D axial T2-layer scans, repeated spherical reconstructions can show nerve-root number, orientation, branches, and leakage source. Skin incision and bone window designs depend on preoperative MRI evaluation. For TCs within nerve roots, the bone window covers the nerve-root length and branches; for cysts without nerve roots, it covers the leakage source.
MRI reconstruction guided by 3D-FIESTA-C enables accurate preoperative assessment of nerve roots in sacral TCs. Combined with intraoperative electrophysiological monitoring, it can protect affected nerve roots, avoid severe deficits, and allow complete cyst resection without complications. MRI reconstruction provides crucial information for optimal sacral TCs surgery.
Selection of surgical approaches and causes of failure
Surgical approaches for sacral TCs include interventional surgeries and open surgeries. Interventional surgeries involve simple cyst aspiration and CT-guided percutaneous aspiration combined with biogel injection. Simple cyst aspiration has a high recurrence rate and is usually only used as a diagnostic treatment. The principle of CT-guided percutaneous aspiration plus biogel injection is that the injected fibrin glue can block the orifice of the leakage, induce cyst wall fibrosis and cyst sclerosis, and prevent cerebrospinal fluid flow, thus achieving symptom improvement. Murphy et al. reported the treatment of 213 patients with sacral TCs using double-needle aspiration plus gel injection [13]. 74% of the patients had good symptom improvement. However, this surgical method is not suitable for sacral TCs. Firstly, there is a high risk of nerve puncture. Secondly, glue injection therapy does not eliminate the space-occupying effect of the cyst. Instead, the hardened biological glue exacerbates the space-occupying effect and causes more severe irritation to the nerve roots within the cyst, aggravating the pain.
The primary options for open surgery mainly consist of autologous fat/muscle-bioadhesive tamponade and partial cyst wall resection combined with nerve root sleeve reconstruction. Compared with interventional puncture, aspiration, and glue filling, this procedure is more secure and reliable in terms of sealing and plugging the leakage.
Most surgeons use partial cyst-wall resection and nerve-root-sleeve reconstruction [14]. During the operation, after incising the cyst, identifying the nerve-root morphology and leakage site, part of the cyst wall is removed. The residual cyst wall is then folded and sutured to reduce leakage and reconstruct the nerve-root sleeve, which remodels the nerve-root anatomy and eliminates the cyst’s space-occupying effect. Domestic and foreign reports confirm this operation’s ideal effect. To reduce recurrence, some scholars fill the leakage with fat or muscle and fix them with the surrounding capsule wall for better sealing. However, high recurrence rates and postoperative complications like symptom aggravation and cerebrospinal fluid leakage have been reported.
Based on the pathogenesis of sacral TCs, this study suggests that the main causes of postoperative recurrence are failure to treat the cystic fistula and inadequate nerve root sleeve reconstruction. The thin cyst walls of most sacral TCs make nerve root sleeve suturing during reconstruction difficult, potentially resulting in an incomplete cuff with insufficient compression resistance. This can lead to cerebrospinal fluid leakage, cyst recurrence, nerve root exposure, and symptoms of nerve root irritation or injury. Previous literature reports that using a nePTFE membrane to surround the cyst after puncture aspiration (without radiculoplasty) to enhance the strength of the nerve root sleeve is a new idea for treating recurrent, symptomatic sacral TCs [15].
Advantages and key elements of reinforced radiculoplasty
In contrast to the traditional method of radiculoplasty, our team used the reinforced radiculoplasty technique to treat postoperative recurrent symptomatic sacral TCs [16]. Based on the traditional technique, we wrapped and strengthened the reconstructed nerve root sleeve with artificial dura mater.
We hold that radiculoplasty is of great significance. Firstly, radiculoplasty restores the normal physiological internal environment of the nerve root and prevents nerve root exposure. Moreover, overlapping sutures can reinforce the congenitally weak cyst wall. Secondly, during the surgery in this study, the diameter of the fistula needs to be enlarged, converting the cerebrospinal fluid unidirectional valve into a bidirectional one, thereby interrupting the cyst’s enlargement mechanismically. Additionally, radiculoplasty alleviates nerve root pain caused by cerebrospinal fluid pulsating against the cyst wall.
Reinforced radiculoplasty of the nerve root sleeve also holds importance. Firstly, before reinforcement, the reconstructed nerve root sleeve may lead to cyst recurrence due to the thin cyst wall. Secondly, a reinforced and reconstructed nerve root sleeve has a high short-term capacity to withstand hydrostatic pressure. Besides, the encapsulated artificial dura mater stimulates the body’s self-repair response. As the artificial dura mater degrades, a dense layer of connective tissue forms outside the nerve root sleeve, encapsulating the nerve root. Consequently, both in the short and long term, the postoperative cyst recurrence rate is reduced and symptoms are effectively relieved.
In the reinforced radiculoplasty, key points include: (1) Nerve root protection: The cyst wall and nerve root are closely related, with nerve root in the cyst potentially adhering to the wall or being part of it, and the sacral nerve often attaching outside. Meticulous nerve root protection is essential to prevent postoperative symptom exacerbation or dysfunction. Electrophysiological monitoring during separation, incision, suture, reinforcement, and reconstruction is crucial. Precise intraoperative monitoring increases the likelihood of maximizing leak and sleeve narrowing, reducing recurrence. (2) Reinforcement materials and tension: The 3D-printed ReDura (Medprin) was used. It has good histocompatibility, strength, and degradability, with a thickness like normal nerve root sleeves. The artificial dura mater’s length is from the cyst leak to the nerve root exit, and its width is 2-3 mm more than the sleeve’s maximum circumference. When suturing, leave a 0.5–1 mm space between the sleeve and cuff. A large space may cause cerebrospinal fluid leakage or recurrence, and a small one may lead to nerve ischemia and edema. (3) Posterior wall of the sacral canal treatment: If the posterior wall of the sacral canal is intact, laminar reduction should be done to restore its structure and maintain pressure, reducing dead space, facilitating muscle attachment and growth, and minimizing deep effusion.
The reinforced radiculoplasty maximized nerve protection and addressed cyst recurrence risk factors. The patient had a good prognosis after the second surgery with no recurrence during long-term follow-up.
There are also some potential complications in the reinforced radiculoplasty. The volume of recurrent cysts is generally large. This means that a huge cavity will be left after the operation. The weak sacrococcygeal muscles and soft tissues, however, are unable to effectively fill this large cavity, which is likely to result in the retention of fluid in the surgical area after the second operation and make the wound even more difficult to heal. To reduce the residual fluid in the surgical area, the patient needs to lie prone in bed for several days after the operation (as the stable hydrostatic pressure in the prone position can reduce the extravasation of liquid), and the wound should be moderately compressed with a 1-kilogram weight.
This study has several limitations. First, due to the small number of cases of postoperative recurrence of symptomatic sacral TCs, this study was only a small retrospective study to initially investigate the efficacy of reinforced radiculoplasty in such patients. In the future, we will conduct a larger prospective cohort study to enhance the persuasiveness of the study. Second, we plan to compare reinforced radiculoplasty with other appropriate surgical methods under unified standards to further verify its advantages and disadvantages, so as to provide more valuable references for clinical treatment.

Comments (0)