
Remember me
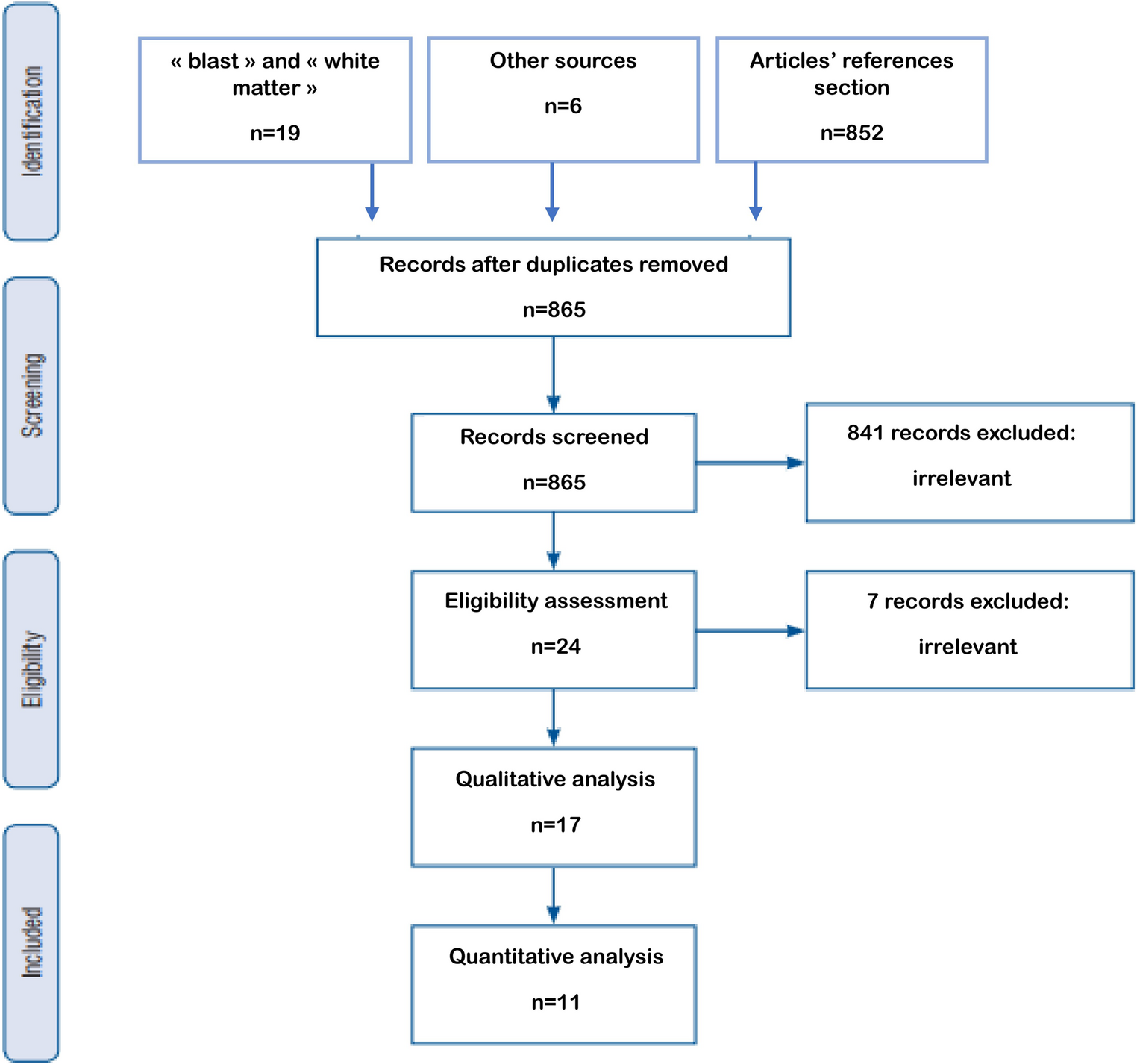
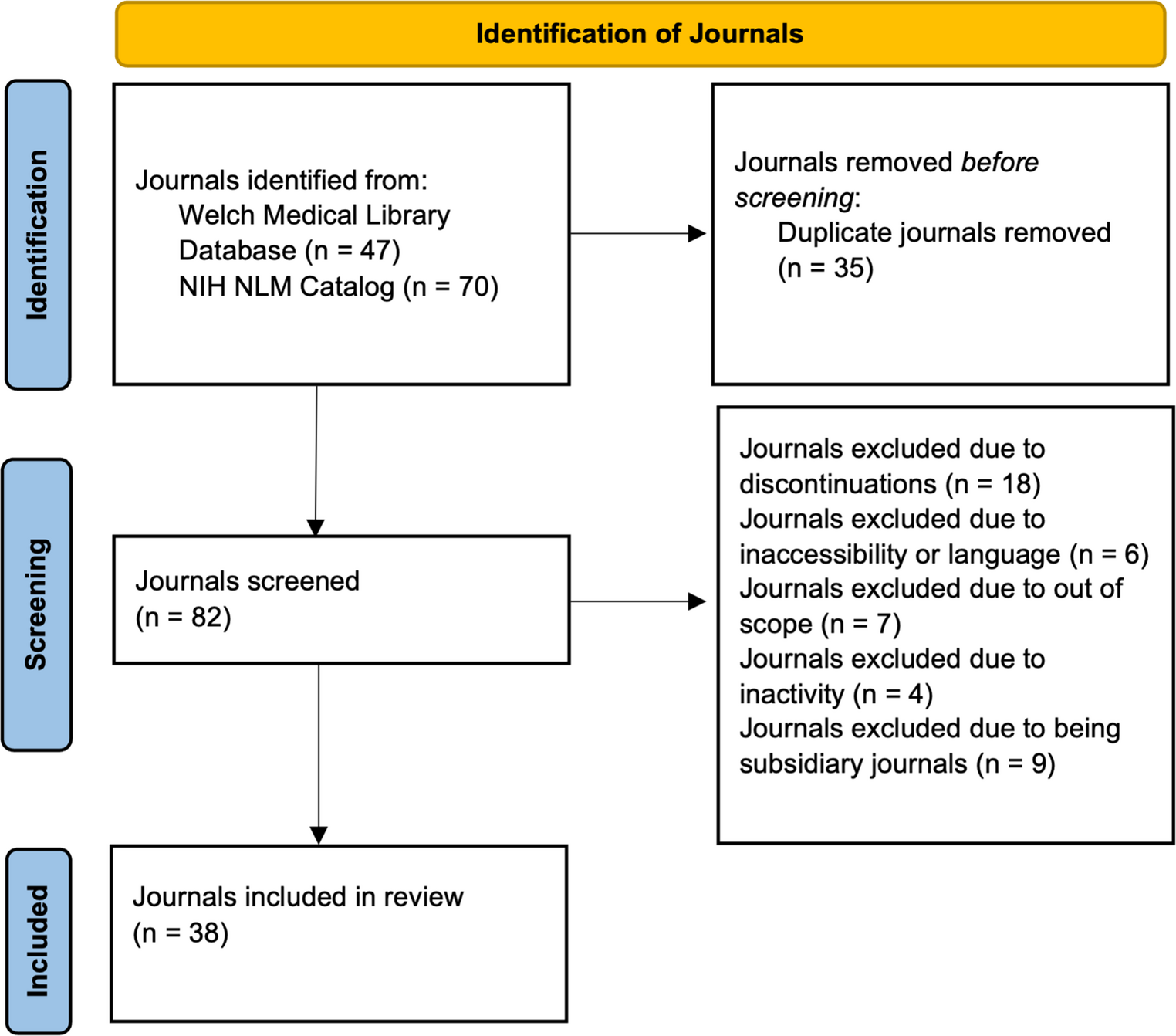
In 74 reports were 53 studies (k) eligible for meta-analysis and 21 for narrative/covariate review (Fig. 1; Table 2) [26,27,28,29,30,31,32,33,34,35,36,37,38,39,40,41,42,43,44,45,46,47,48,49,50,51,52,53,54,55,56,57,58,59,60,61,62,63,64,65,66,67,68,69,70,71,72,73,74,75,76,77,78,79,80,81,82,83,84,85,86,87,88,89,90,91,92,93,94,95,96,97,98,99]. Overlapping populations were seen in 14 reports but most described different outcomes and only two were excluded from the meta-analysis [41, 69]. All studies were observational and apart from two all were retrospective [68, 85]. Reports originated mainly from European (k = 35), Asian (k = 22) or North American (k = 12) continents. Countries of origin included Germany (k = 14), United States of America (k = 12) and China (k = 8). Most studies (89%) were of surgical cohorts and the remainder had radiosurgery. Any grade of meningioma was included in most (75%). Inclusion years ranged from 1968 to 2023; most (58%) recruited within the previous 10 years. Most patients were female in the 6th or 7th decade of life. Preoperative oedema was seen in 49% of patients (k = 40, total n = 10,124). Oedema was identified by magnetic resonance imaging (MRI) in 72% of studies with a binary (55%) or threshold (32%) definition. Prophylactic ASM use was specified in 55% of reports; of which 49% of studies used them (ranging from 9 to 100% of patients), 41% did not, and the remainder (10%) had preoperative seizures (Online Resource 3). In studies that provided seizure proportions, 23% of patients had preoperative seizure (k = 30, total n = 7,785), 6% had early postoperative seizure (k = 8, n = 2,873), and 17% had late postoperative seizures (k = 9, n = 2,150). A description of seizure semiology, outcome, or definition was provided in 27% of reports (Online Resource 3). Pre-operative focal seizures were identified in 27–65% of patients with seizure (impaired awareness in 2–14%) and 36–51% had new postoperative focal seizures. Generalised seizures were noted in 34–68% preoperatively and new generalised seizures in 32–55% postoperatively. Most studies report long-term postoperative seizure freedom (Engel I or ILAE classification I) in approximately 80–90% of patients, decreasing to 70–80% in those with preoperative seizures. Many studies had a high risk of bias due to confounding factors or measurement of oedema (Fig. 2).
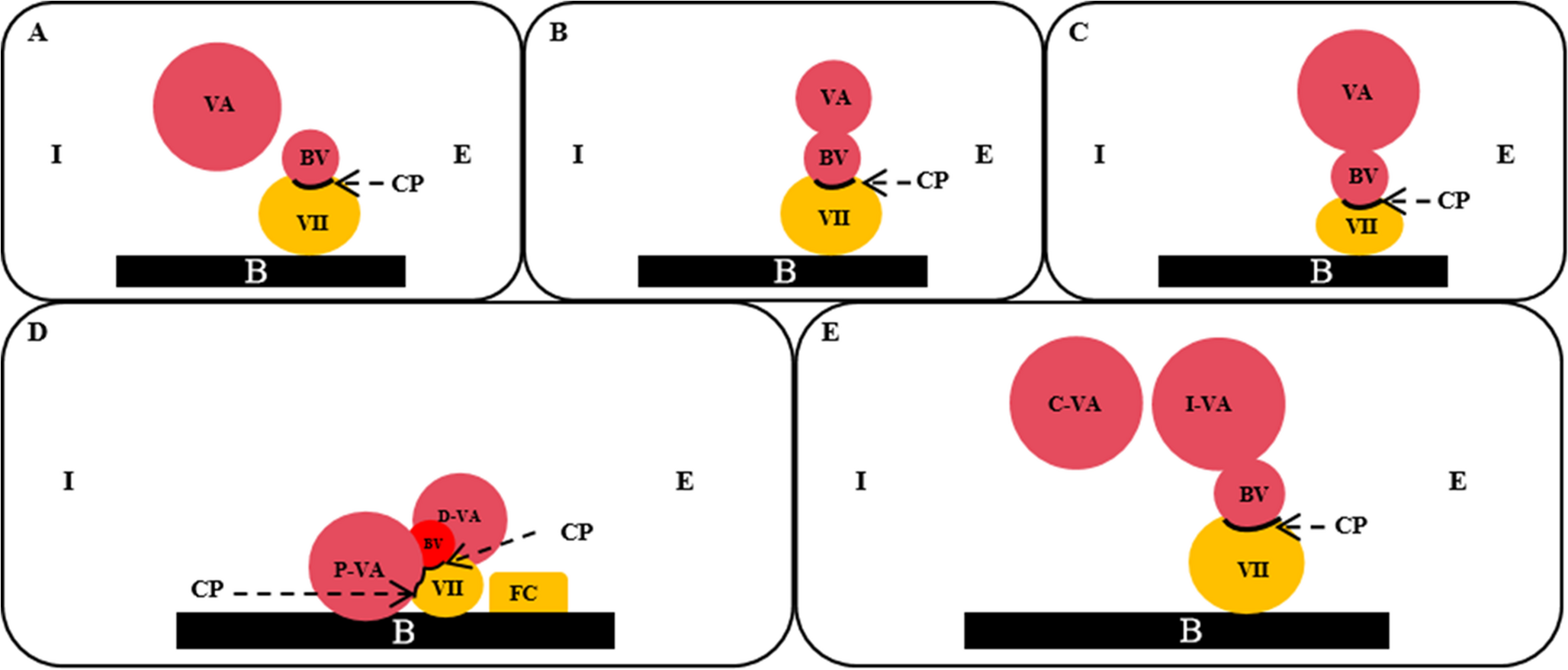
Table 2 Details of included studies Fig. 2
Risk of bias assessments: A Preoperative oedema and seizure; B Preoperative oedema and early postoperative seizure; C Post-radiosurgery oedema and seizure; D Preoperative oedema and late postoperative seizure; E Seizure and postoperative oedema; F Preoperative oedema and any postoperative seizure
Preoperative oedema and preoperative seizuresIn our meta-analysis, preoperative oedema significantly increased the odds of preoperative seizure (k = 32, n = 8,345, OR 3.6, 95% CI = 2.6–4.9, I2 = 67%, Fig. 3). Only 13% of patients without oedema had seizure, whilst 34% with oedema had seizure. Heterogeneity was moderate, rectified by removal of outlying studies (k = 28, n = 7,725, OR 3.5, 95% CI = 3.1–4.0, I2 = 0%, Online Resource 4, GRADE: high). In our covariate review preoperative oedema was a significant predictor of preoperative seizure in univariable (95%, k = 21) and multivariable analysis (81%, k = 16) (Online Resource 5 and 6). Stevens et al. proportioned seizure semiology in patients with oedema: focal − 50%, grand mal – 26% [83]. Chaichana et al. found oedema to be unrelated to uncontrolled preoperative seizures [99]. Seven additional studies (not eligible for meta-analysis or covariate review) described relationships between preoperative oedema and preoperative seizures with mixed results (Online Resource 7).
Fig. 3
Forest plot of preoperative oedema and preoperative seizure, unadjusted with outliers
Preoperative oedema and postoperative seizuresThere were 28 eligible studies for meta-analysis of preoperative oedema and postoperative seizure: nine early (< 1 week), nine late (> 1 week) and 15 unclear. Oedema was associated with early postoperative seizures (k = 9, n = 2,929, OR 1.5, 95% CI = 1.1–1.9, I2 = 0%, Fig. 4A, GRADE: moderate). There were no outliers. Proportions with seizure increase from 5 to 8% when oedema is seen. Two additional studies were suitable for narrative review (Online Resource 7) with contrasting conclusions. Oedema was significantly associated with late postoperative seizures (k = 9, n = 2,150, OR 1.9, 95% CI = 1.5–2.2, I2 = 0%, Fig. 4B, GRADE: moderate). Proportions with seizure increase from 13 to 20% when oedema was present. There were no outliers. We pooled postoperative seizure studies and selected unique subsets from each study (Online Resource 8). Preoperative oedema increased risk of postoperative seizure (k = 32, n = 8,181, OR 1.6, 95% CI = 1.4–2.0, I2 = 65%). Postoperative seizure proportions increase from 10 to 18% with preoperative oedema. Outlier removal results in low heterogeneity (k = 31, n = 7,776, OR 1.8, 95% CI = 1.5–2.1, I2 = 10%, GRADE: moderate, Online Resource 4). Seizures could have occurred any time within postoperative follow up (one to 286 months, Online Resource 8) but two studies specified seizure outcome at 3 or 12 months postoperatively [69, 77]. In covariate review, oedema was seldom a predictor for seizures in univariable analyses (Early: 14% of seven studies, Late: 20% of five studies, All: 44% of 16, Online Resource 5) and multivariable analyses (Early: 33% of three studies, Late: 33% of three studies, All: 22% of nine, Online Resource 6). There was no association between preoperative oedema and refractory epilepsy in one study [82].
Fig. 4
Forest plot of: A preoperative oedema and early postoperative seizure, B preoperative oedema and late postoperative seizure
Radiotherapy and seizuresEight studies reported oedema and seizure following radiosurgery (Online Resource 9). Post-treatment oedema occurred in 15%, and 4% had post-treatment oedema and seizure. It is unclear whether oedema precedes seizures in these reports. Two studies noted oedema occurring an average of seven months after CyberKnife treatment [29, 73]. In our meta-analysis, post-radiosurgery oedema was not associated with post-radiosurgery seizure (k = 3, n = 376, OR 10.9, 95% CI = 0.6–211.3, I2 = 42%, GRADE: very low, Fig. 5). Proportions of seizure in patients with post treatment oedema was 6% compared to 2% without.
Fig. 5
Forest plot of post radiosurgery oedema and seizure
Other associations between oedema and seizuresPaediatricIm et al. studied 10 children (median age eight years) with operated meningioma [46]. They found no association between preoperative oedema and preoperative seizure (OR 1.0, 95% CI 0.1–12.6) or postoperative seizure (OR 0.4, 95% CI 0.1–12.6) [46]. Some studies did include paediatric patients, but only three specified proportions (range 1.4–6.0%, Table 2), so Im et al. was excluded from the meta-analyses. For sensitivity analysis we repeated our meta-analyses with Im et al. Results were similar for preoperative oedema and seizure (k = 33, n = 8,355, OR 3.5, 95% CI = 2.6–4.8, I2 = 66%). Results were also similar for preoperative oedema and unknown postoperative seizure with Im et al. (k = 16, n = 4,639, OR 1.8, 95% CI = 1.5–2.3, I2 = 79%) and without (k = 15, n = 4,629, OR 1.9, 95% CI = 1.5–2.4, I2 = 80).
Postoperative oedemaSix studies noted postoperative oedema. Preoperative seizure was not significantly associated with new/worsening postoperative oedema, but postoperative seizures and postoperative oedema were associated (Online Resource 4).
Subgroup analysis and meta-regressionWe performed subgroup analysis (minus outliers) and meta-regression for preoperative oedema and preoperative or (any) postoperative seizure (Online Resources 10 to 15). For preoperative seizure there was no difference by continent of study, inclusion of infratentorial tumour, imaging modality used for oedema, oedema measurement, or use of seizure definition. Very high risk of bias was associated with an inflated OR and subgroup difference (Online Resource 10), but there was no significant difference in meta-regression (Online Resource 12 and 13). We subset studies of postoperative seizure by preoperative seizure status (Online Resource 8). For preoperative oedema and postoperative seizure, there were no differences with risk of bias, preoperative seizure status, postoperative seizure status (early versus late), infratentorial tumour inclusion, continent, imaging modality, oedema measurement, and with prophylactic ASM use (any proportion) in seizure naïve patients.
Publication biasFunnel plots and Egger’s test suggested publication bias for preoperative oedema and all postoperative seizures (Fig. 6B, Online Resource 4). This was resolved on outlier removal as demonstrated by repeat funnel plots, Egger’s test and p-curve analysis (Online Resource 4 and 16). There was no evidence of publication bias for other analyses.
Fig. 6
Funnel plots for meta-analyses of: A Preoperative oedema and preoperative seizure; B Preoperative oedema and postoperative seizure; C Preoperative oedema and early postoperative seizure; D Preoperative oedema and late postoperative seizure; E Post radiosurgery oedema and seizures; F Preoperative seizure and postoperative oedema; G Postoperative seizure and postoperative oedema and (H) Preoperative oedema and seizure (adjusted). Grey circle denotes study, green cross denotes outliers, and red triangle denotes simulated study using trim and fill
Covariate reviewWe noted all non-oedema seizure predictors in univariable and multivariable tests (Online Resource 5 and 6). Factors associated with preoperative seizures included falcine (100%, k = 3) or parasagittal locations (60%, k = 5), brain invasion (60%, k = 5) and oedema (95%, k = 21). Negative associations included headache (83%, k = 6), preoperative deficit (71%, k = 7) and skull base tumours (67%, k = 9). On multivariable analyses only oedema (81%, k = 16) was consistently reported as a positive and headache (100%, k = 6) a negative predictor.
For any postoperative seizure, preoperative seizures (85%, k = 13), postoperative deficit (67%, k = 6) and tumour recurrence (67%, k = 9) were significant. In multivariable testing, only presence of com
Comments (0)