
Remember me



In 2023, five subjects were enrolled from the Valduce Hospital – Villa Beretta Rehabilitation Center (Costa Masnaga, Italy) and the INAIL network (Istituto Nazionale Assicurazioni Infortuni sul Lavoro, National Institute for Industrial Accidents Insurance, Italy). All participants provided written informed consent. The research protocol was approved by the ethics committee of IRCCS Medea (Prot.N. 14/22 -CE, approved on February 17, 2022). The study protocol was retrospectively registered on clinicaltrials.gov (NCT06321172).
The recruitment followed health and safety criteria to ensure proper and safe use of the FES-cycling device.
Inclusion criteriaAge between 18 and 65 years.
Paraplegia resulting from a SCI (both traumatic and non-traumatic) that occurred less than five years prior to the study to facilitate muscle conditioning.
Complete loss of motor function in the lower limbs (level ≤ T3, ASIA A or B) with residual trunk control.
Sufficient muscle contraction using FES with surface electrodes to effectively use the device.
Exclusion criteriaSevere osteoporosis with an elevated fracture risk as assessed by an expert clinician.
Severe spasticity and pain preventing device use.
Skin lesions in areas interfacing with the trike.
Dysfunction of the autonomic nervous system.
Psychopathological comorbidities.
Fig. 1
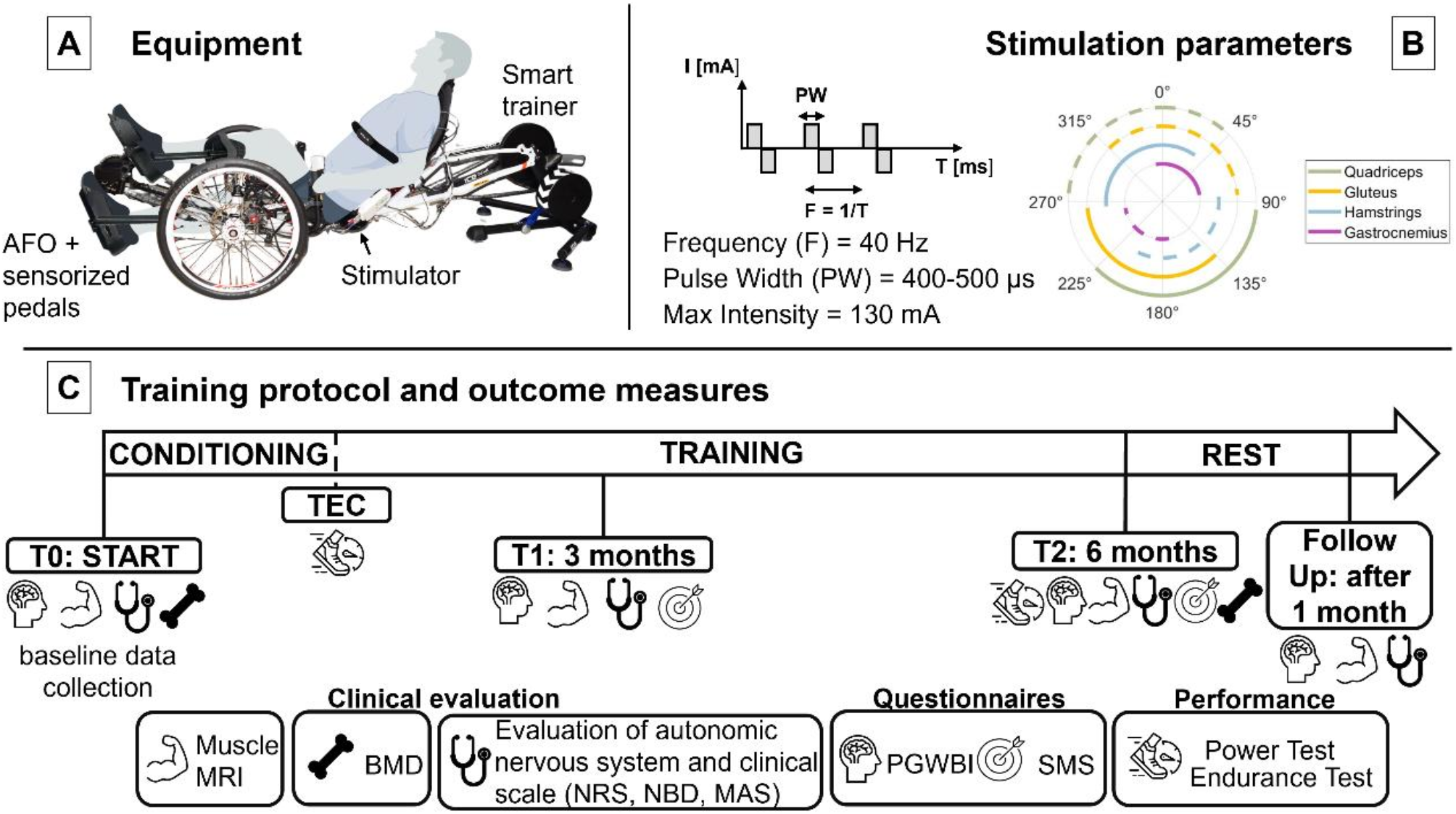
Description of the equipment and stimulation strategy used during the study. (A) Schematic representation of the set-up (composed on BioRender.com) while (B) definition of the stimulation parameters used during the training protocol. In (C) the training protocol followed in the study is presented together with the outcome measures. Definition of acronyms: Ankle-Foot Orthosis (AFO), time at the end of the conditioning phase (TEC), Magnetic Resonance Imaging (MRI), Bone Mineral Density (BMD), Numerical Rating Scale (NRS) Neurogenic Bowel Dysfunction (NBD), Modified Ashworth Scale (MAS), Psychological General Well-Being Index (PGWBI) and Sport Motivation Scale (SMS)
EquipmentThe device used in this study is a prototype developed by Politecnico di Milano, based on a commercial recumbent trike (ICE VTX, 2017), and specifically adapted for FES-cycling for individuals with reduced mobility [23] (see Fig. 1A).
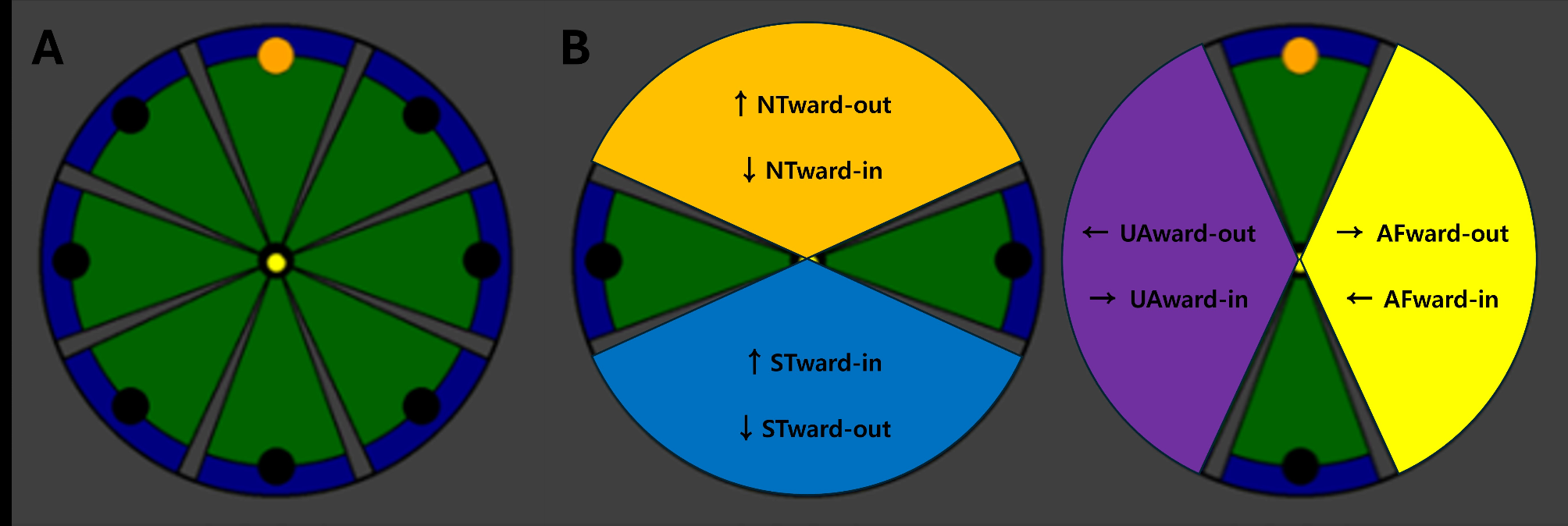
The system uses two battery-operated four-channel stimulators (RehaMove3, Hasomed GmbH) to activate four muscles in each leg through surface self-adhesive electrodes (Pals® from Axelgaard Manufacturing Co. Ltd.). The stimulators deliver balanced biphasic current pulses to the gluteus, quadriceps, hamstrings, and gastrocnemius muscles in both legs. Pulse duration is set at 400–500 µs, frequency at 40 Hz, and current amplitude up to 130 mA, individually calibrated for each participant. The stimulation parameters are selected based on their widespread use in literature for FES applications [6]. The stimulation amplitude is automatically adjusted using a Proportional-Integral (PI) controller to maintain a consistent cadence [30]. A magnetic absolute rotative encoder (AS5047P, ams OSRAM) measures the crank angle, allowing for the sequential activation of muscles during specific angular ranges of the cycling motion (see Fig. 1B).
Users interact with the system through four buttons and a 7-inch touchscreen display, which also provides information on stimulation settings and training sessions.
The system includes custom-made ankle foot orthoses (AFOs) to stabilize leg movement. These are attached to two commercial sensorized pedals (X-Power, SRM GmbH) integrated into the system, which measure power output during exercise.
This setup is suitable for both outdoor and indoor use. For indoor training sessions, the back wheel is replaced with a KICKR smart trainer.
Protocol and outcome measuresAt the beginning of the study, baseline data were collected, including demographic information (age, gender, height, weight), injury-related details (level of injury, time since injury, American Spinal Injury Association scale - ASIA), and prior experience with FES and/or cycling/trike use post-injury. The outcome measures were collected at different time-points (see Fig. 1C):
T0: start of the study.
TEC: end of the conditioning phase.
T1: 3 months from the beginning of the study.
T2: 6 months from the beginning, at the end of the training.
Follow up: 1 month after the end of the training.
The primary outcome was the Cross-Sectional Area (CSA) of thigh muscles, assessed using Magnetic Resonance Imaging (MRI) at T0, T1, T2, and follow-up. The secondary outcome measures are detailed below:
Dual-energy X-ray absorptiometry (DXA) for measuring bone mineral density (BMD) and assessing bone health. Timepoints: T0 and T2.
Blood pressure (BP), heart rate (HR) and hemodynamic parameters for evaluating the autonomic nervous system. Timepoints: T0, T1, T2 and follow up.
Modified Ashworth Scale (MAS) [37] to assess spasticity of the lower limbs. Timepoints: T0, T1, T2 and follow up.
Neurogenic Bowel Dysfunction (NBD) score [38] to evaluate intestinal function. Timepoints: T0, T1, T2 and follow up.
Numerical Rating Scale (NRS) [39] to quantify subjective evaluation of perceived pain levels. Timepoints: T0, T1, T2 and follow up.
Psychological General Well-Being Index (PGWBI) [40] questionnaire to evaluate the impact of continuous FES-cycling on participants’ well-being. Timepoints: T0, T1, T2 and follow up.
Sport Motivation Scale (SMS) [41] to assess drivers’ motivation for participating in sports. Timepoints: T1 and T2.
Power produced while cycling at maximum current amplitude to evaluate maximal power output. Timepoints: TEC and at T2.
Maximum distance traveled in six minutes to assess endurance. Timepoints: TEC and at T2.
Pilots were asked to achieve a minimum compliance rate with the protocol, which required them to attend at least 75% of the training sessions in the six months.
Muscle evaluation using MRIFour out of five volunteers were scanned using a Philips Achieva dStream 3T MRI scanner with a torso coil, utilizing a T1-weighted (T1-w) turbo spin echo sequence (pixel size: 1 × 1 mm2; slice thickness 6 mm, no gap; number of slices: 50; Matrix: 256 × 256; Echo Time: 15ms; Repetition Time: 600ms; flip angle: 90°; SENSE: 2; Number of averages: 2). Due to a spinal cord implant not compatible with MRI scans at 3T, one volunteer was scanned using a General Electric 1.5T MRI scanner with an 8-channel body FullFOV coil. A T1-w fast spin echo sequence was performed (pixel size: 1 × 1 mm2; slice thickness 6 mm; number of slices: 50; Matrix: 256 × 256; gap: 9 mm; Echo Time: 13.3 ms; Repetition Time: 600ms; flip angle: 90°; Number of averages: 1). All sequences were acquired on one thigh, with the field of view extending to the middle of the femoral head.
To derive CSA, regions of interest (ROIs) were delineated for specific thigh muscles, including the vastus lateralis, vastus medialis, vastus intermedius, rectus femoris, sartorius, gracilis, adductor magnus, semimembranosus, semitendinosus, biceps femoris caput longum, biceps femoris caput breve, and adductor longus. The segmentation was guided by a reference range, from the beginning of the semimembranosus to the last available slice of the rectus femoris. Consistency was maintained in the ROIs across all longitudinal scans for each participant [42]. ROIs were semi-automatically traced on T1-w images using the Dafne tool (Deep Anatomical Federated Network), which is accessible at https://dafne.network/ [43]. This process entailed an initial automated outline, which was then meticulously refined by users via an interactive interface. The maximal CSA (maxCSA) was determined by identifying the slice showing the largest muscle cross-sectional area.
Bone health evaluation using DXABMD measurements were performed using the HOLOGIC QDR 4500 system (Hologic, Inc, USA) to assess osteoporosis and derive T-score parameters. The T-score classifies bone condition, with values above − 1 indicating normal bone density, between − 1 and − 2.5 indicating osteopenia, and below − 2.5 indicating osteoporosis. Standard protocols were used for the column and femoral neck, resulting in 2 T-score values. The Toronto Rehab Protocol [44] was applied to the distal femur and proximal tibia, yielding 8 T-score values per leg, for a total of 18 T-scores per subject.
Evaluations of the autonomic nervous systemThe autonomic nervous system was evaluated using the Task Force® Monitor (CNSystems Medizintechnik GmbH, Austria), which provides continuous recording of systolic and diastolic blood pressure (sBP and dBP), HR and the total peripheral resistance index (TPRI).
The assessment involved a series of tests commonly employed in clinical practice to simulate the stress conditions typically experienced by the cardiovascular system during daily activities. The tests included:
Supine position evaluation for 3 min, which is considered as the rest condition.
Tilt-up test: passive verticalization by tilting the bed from a flat position to 60°, held for 5 min.
Stepping in place with an automatic step induction system (Erigo, Hocoma) at a cadence of 60 steps per minute for 5 min.
Passive cycling for 5 min using the LAMBDA system (Lambda Health System, Switzerland) to assess the impact of cycling on the autonomic nervous system. The LAMBDA System is a parallel robot that may be used for mobilization of the lower extremities, simulating different motor tasks, including cycling. This device was chosen because it can resemble the task performed by participants during the training sessions.
The mean values of HR, dBP, sBP and TPRI were computed for each pilot during each specific test (Rest, Tilt-up, Stepping and Lambda).
Clinical scalesClinical evaluations of the level of spasticity of the lower limbs, intestinal function and a subjective assessment of the level of pain perceived by the subject were carried out. In particular:
The MAS was used to evaluate the severity of spasticity, measuring the velocity-dependent resistance of a muscle to passive stretch. The scale ranges from 0 to 4, where 0 indicates no increase in muscle tone and 4 denotes a rigid joint limb.
The NBD score was used to evaluate symptoms related to bowel management and function, including constipation, incontinence, and the impact on daily life. The NBD tool consists of 10 questions, each assigned specific point values. The maximum possible score is 47, where a score above 14 indicates severe bowel dysfunction.
The NRS was used to measure the intensity of general pain experienced by the pilots in their daily lives, with 0 indicating no pain and 10 representing high pain.
Well-being evaluationPGWBI is a self-report questionnaire designed to assess overall psychological well-being. It is composed by 22 items that investigate 6 different dimensions: Anxiety, Vitality, Depression, Self-control, Positivity and Vitality. Each question is scored on a scale from 0 to 5, with a total score ranging from 0 (indicating maximum distress) to 110 (indicating maximum well-being). The PGWBI questionnaire was administered to assess the impact of continuous FES-cycling activity on participants’ well-being.
Evaluation of the sport motivationSMS is a tool used to evaluate an individual’s motivation for participating in a sport activity. It measures different types of motivation, including intrinsic (enjoyment and personal satisfaction) and extrinsic (rewards and recognition) factors, as well as amotivation (lack of motivation). The SMS consists of 28 questions divided into seven subscales, each reflecting a different type of motivation: Intrinsic Motivation to Know, Intrinsic Motivation to Accomplish, Intrinsic Motivation to Experience Stimulation, Identified Regulation, Introjected Regulation, External Regulation and Amotivation. Each question is rated on a 7-point Likert scale, where 1 corresponds to strongly disagree, while 7 strongly agree. Participants were asked to focus on FES-cycling on a recumbent trike when answering the questions to assess their perception of the training as sport-therapy.
Performance evaluationTwo tests were conducted on the recumbent trike to assess the impact of the training on performance: a maximal power test and a cycling endurance test. In the maximal power test, the sensorized pedals measured the peak of power output produced by the pilots while providing them with the maximal current amplitude for 2 min. In the cycling endurance test, the maximum distance traveled in 6 min was computed. During the endurance test, the stimulation intensity was automatically adjusted by the PI controller.
Training modalitiesOver six months, each participant engaged in biweekly FES-cycling training sessions, lasting up to 30 min of stimulation. The training period was mainly conducted indoors at the Politecnico di Milano, under the supervision of clinical staff from the IRCCS Medea, using the KICKR smart trainer set to 10% resistance. The experimental protocol began with a conditioning phase where stimulation and trike parameters were tailored to each participant’s individual needs. This phase aimed to train the leg muscles to enable independent pedaling for at least six minutes, assisted solely by FES. If participants were unable to complete a training session during the conditioning phase, operators provided manual assistance. The duration of the conditioning phase varied depending on individual progress, ensuring participants were adequately prepared for the required effort during training. Once the conditioning phase was successfully completed, the main training period commenced. Each training session included a 3-minute warm-up, four sets of 6-minute pedaling intervals, and a 3-minute cool-down, with a pedaling cadence maintained between 20 and 50 RPM, with no manual assistance from the operator, relying solely on FES-supported pedaling.
To incorporate a recreational aspect, participants also engaged in occasional outdoor cycling sessions. These sessions aimed to foster the enjoyment and motivational benefits of cycling in a non-clinical setting. Furthermore, some participants had the opportunity to participate in parallel events such as the Lyon Cyber Days and the Cybathlon Challenges 2024, highlighting the integration of sportive and community-based activities alongside structured training program.
Statistical analysisThe sample size of five subjects was chosen due to the pilot nature of the study and the 6-month protocol, deemed sufficient to provide preliminary evidence of the muscle-level efficacy of FES-bike training. The data were analyzed using IBM SPSS Statistics v21 and MATLAB (R2023a), with a significance level set at 5%. Descriptive statistics were used for demographic data analysis.
For all outcome measures but DXA assessments, the Wilcoxon test was applied for comparisons between two timepoints, while the Friedman test was used for comparisons across multiple timepoints. If significant differences were detected, post-hoc analysis using Bonferroni correction for significance. For DXA assessments, an intrasubject Wilcoxon test compared T0 and T2 assessments using the 18 T-scores per subject.
Changes in the primary outcome (muscle maxCSA) after 6 months were correlated with performance outcomes (peak power and distance travelled) using Spearman’s Rho.
All outcome measures were reported as median values with interquartile ranges.
Comments (0)