As outlined in the introduction, this study explores two primary themes. First, the results from W0 to W4 reflect the effects of each intervention—RT, BTX, or RT + BTX. Second, the results from W0 to W8 examine the effects based on the timing of each intervention.
Effects of each RT or BTX: results from W0 to W4
From W0 to W4, no significant Time × Group interactions were observed in the FMA across any of the groups. Regarding kinematic-whole measures, Group B0R0 demonstrated significant Time × Group interactions in all kinematic-whole measures, Group B0R4 showed significant interactions in three kinematic-whole measures, and Group B4R0 showed significant interactions in just one kinematic-whole measure compared to Group B4R4. Furthermore, Group B0R0 exhibited the greatest number (9) of significant Time × Group interactions in kinematic-IND measures.
In terms of spasticity, significant Time × Group interactions in MAS-EF were observed in Groups B0R0 and B0R4, whereas Groups B4R4 and B4R0 did not show any significant Time × Group interactions. This suggests that significant spasticity reduction occurred only in the groups receiving BTX, indicating that RT alone was insufficient to reduce spasticity. Although the W4 to W8 data are not included here, significant changes in MAS-EF were also observed in Groups B4R4 and B4R0 from W4 to W8. These results demonstrate that spasticity improvements were primarily achieved through BTX rather than RT. Similar findings were reported by Pennati et al., who found that spasticity reduction was significantly greater with BTX compared to RT [9].
The effects of RT may vary depending on the type of rehabilitation robot or the training method used. A previous study comparing two training methods with the same robot used in our study—one similar to ours (upper limb movement regardless of flexion or extension) and the other focusing on extensor training—found no change in elbow spasticity in either group [24]. However, non-specific RT improved passive elbow ROM, while extensor-focused RT enhanced active elbow extension. These findings suggest that if RT had focused more on extensor movements alongside BTX injections, the synergistic effects might have been more pronounced. This is because the relaxed extensors, following BTX administration, could benefit more from robotic facilitation of extensor movement. As robotic rehabilitation continues to advance, more personalized training tailored to individual user characteristics and the specific mechanisms of the rehabilitation robot is likely to be more effective [25, 26].
Effects of timing of RT and BTX injection: results across W0, W4, and W8
Throughout the entire intervention phase (across W0, W4, and W8), only Group B0R4 demonstrated a significant Time × Group interaction in the FMA compared to Group B4R4. For kinematic-whole measures, Group B0R4 showed significant Time × Group interactions in all kinematic-whole measures. Group B0R0 exhibited significant interactions in two measures and Group B4R0 in one. Additionally, Group B0R4 had the highest number of significant Time × Group interactions in kinematics-IND, followed by Group B0R0, whereas Group B4R0 did not show any significant interactions in kinematics-IND. Elbow spasticity, however, did not show any significant Time × Group interactions, suggesting no difference in spasticity across the groups. In summary, Group B0R4 achieved the most effective motor function recovery, followed by Group B0R0, Group B4R0, and finally Group B4R4, with no differences in spasticity observed.
Given that the total amount of RT was identical for all participants, the timing of RT relative to the BTX injection was crucial. BTX typically reaches peak efficacy in reducing muscle spasticity approximately two weeks post-injection, and Group B0R4 received RT when BTX effects were at their peak. Thus, at the time of RT, Group B0R4 likely experienced the greatest reduction in spasticity attributable to BTX, followed by Group B0R0 with a moderate reduction. Group B4R0 may not have experienced any spasticity reduction from BTX. Consequently, the effectiveness of RT was influenced by the degree of spasticity present during RT sessions. RT yielded the most effective results on motor function when the effects of BTX were maximized.
The link between spasticity reduction and motor function recovery can be understood as follows: Participants who experienced greater spasticity alleviation from BTX were likely to have more opportunities for motor learning, as spasticity affects motor learning capability [27]. Additionally, resistance from spastic muscles can hinder robotic-assisted movements during RT. Therefore, spasticity reduction allows for more harmonious movement, as intended by RT, with fewer conflicts between the participants and the robot. A usability test from an upper limb robotic rehabilitation study found that the assistive force from the robot caused conflicts with participants’ spasticity, providing resistance against intended voluntary movements. Thus, more coordinated movements were possible with decreased spasticity [12]. In our study, the intervention dose (number of repetitions) of RT was identical for every participant, and this more coordinated interaction between the human and robot might have influenced the results. Optimal timing of RT during peak BTX effect could enhance neuroplasticity and lead to better integration of new motor skills.
Notably, Group B0R4 demonstrated improvements in SPARC, HPRatio, and MovDev, along with improvements in MeanSp, indicating that the improvements in Group B0R4 led to faster, more efficient, and accurate performance without a speed-accuracy trade-off. This suggests that improvements in one aspect (e.g., smoothness, accuracy) were not counterbalanced by deteriorations in another aspect (e.g., speed). Therefore, the optimal application of interventions, considering the mechanisms of each intervention, can promote motor skill learning and maximize functional gain [28, 29].
Kinematic analysis
Our results were robust owing to the incorporation of kinematic analysis, which provides objective and sensitive assessments of movement in individuals with stroke [30,31,32]. Our study demonstrated that robotic kinematic assessments provided more sensitive and detailed information, including movement smoothness, speed, efficiency, and accuracy, which clinical measurements alone could not offer. Notably, we analyzed not only the overall kinematic data (kinematic-whole measures) but also data segmented by direction, allowing for in-depth information. There were variations in kinematic variables depending on specific movements, aligning with a previous study [12]. This likely reflects that the participants experienced differential difficulty owing to their ULS. Additionally, the differential change depending on the movement showed that the effects of intervention varied across various movements. Therefore, kinematic analysis methods in this study provided a more informative picture reflecting individualized pathophysiology and recovery patterns of participants with stroke.
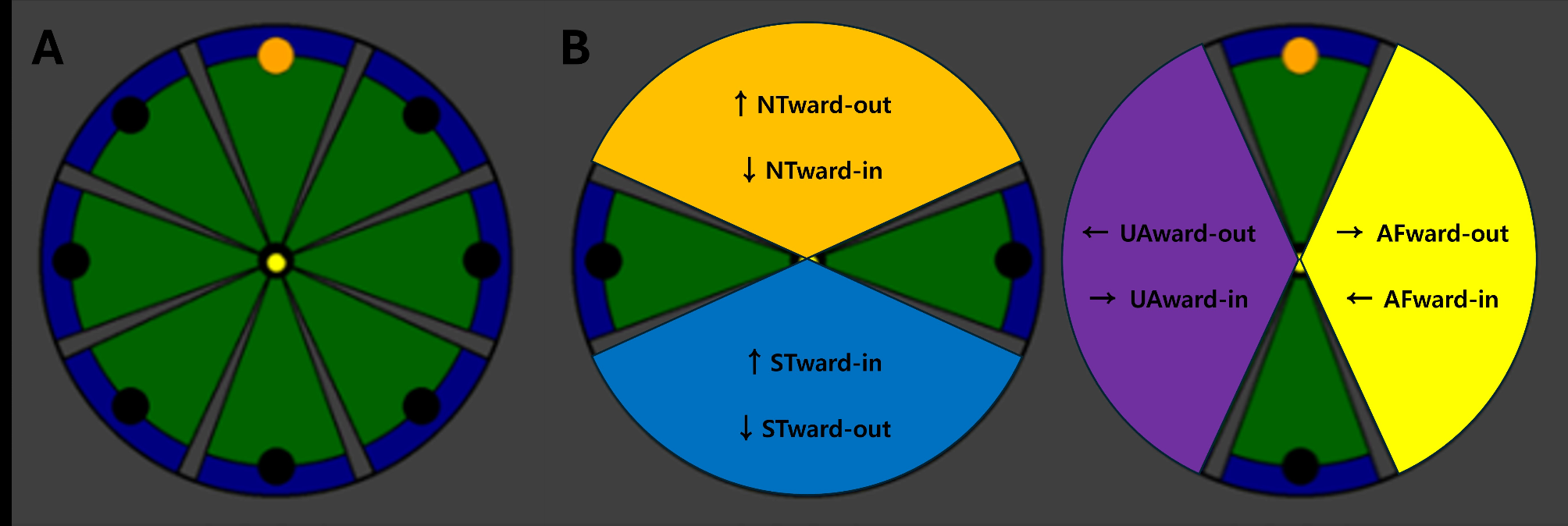
Particularly, the NTward-out and STward-in movements best reflect the effects of our intervention, as they require both a decrease in elbow flexor spasticity and sufficient voluntary elbow extensor activation to counteract flexor spasticity. For NTward-out, significant Time x Group interactions were not observed from W0 to W4 in any groups but emerged from W0 to W8 only in Group B0R4. Similarly, STward-in, which requires elbow joint movement similar to NTward-out but to a lesser extent, showed comparable trends. From W0 to W4, Group B0R0 showed significant Time x Group interactions in SPARC-STward-in and HPRatio-STward-in. From W0 to W8, significant Time x Group interactions in SPARC-STward-in and HPRatio-STward-in were maintained, and a significant Time x Group interaction in MovDev-STward-in emerged in Group B0R0.
Moreover, the inclusion of multiple kinematic variables provided additional insights. We hypothesized that movement smoothness would be the most representative outcome variable, as it is known to have stronger correlations with motor performance than other kinematic measures and has demonstrated greater sensitivity in detecting motor improvements [12, 13, 25, 33]. Concordantly, smoothness, which was represented by SPARC, demonstrated significant findings in the present study. Significant interactions were observed in Group B0R0 from W0 to W4, as well as in Group B0R0 and primarily Group B0R4 across W0, W4, and W8. These findings highlight the complementary roles of BTX and RT in rehabilitation, with BTX establishing the physiological foundation by reducing spasticity and RT subsequently enhancing motor control to facilitate smoother movement. The timing of these interventions was critical, as demonstrated by the superior outcomes in Group B0R4. These significant findings in smoothness are especially meaningful because it is known as a key indicator of upper limb impairment and recovery among individuals with stroke [34].
HPRatio, reflecting movement efficiency, showed a similar pattern to SPARC. From W0 to W4, HPRatio-Whole improved in Groups B0R0 and B0R4; however, only Group B0R0 exhibited significant changes in individual movements. This highlights the importance of BTX-driven spasticity reduction in enabling smoother motion and minimizing resistance during movement execution. Across W0, W4, and W8, HPRatio-Whole improved in Groups B0R0, B0R4, and B4R4, with the most frequent individual movement improvements in Group B0R4, followed by Group B0R0, and none in Group B4R4. This suggests that RT is most effective when timed with sufficient spasticity reduction. BTX optimizes the motor learning environment by reducing spasticity, thereby enhancing robotic interaction and improving movement efficiency.
For MeanSp, a significant improvement in MeanSp-Whole from W0 to W4 was observed only in Group B0R0, while a significant improvement in MeanSp-Whole from W0 to W8 was observed in Group B0R4. Thus, the improvements in MeanSp-Whole in Groups B0R0 and B0R4 can be interpreted as meaningful fundamental changes resulting from the synergistic effects of RT and BTX, as well as the specific mechanisms of action of each intervention. Meanwhile, MeanSp exhibited distinct temporal patterns. From W0 to W4, significant Time × Group interactions were observed in MeanSp, differing from other kinematic variables, including smoothness, efficiency, and accuracy. This speed-accuracy trade-off is commonly encountered, and the improvements from W0 to W4 could be understood as not being generalized to the whole aspects of movement [35]. Interestingly, across W0, W4, and W8, significant Time x Group interactions were consistently observed for all kinematic variables, indicating that improvements in speed did not come at the expense of movement smoothness, efficiency, or accuracy.
These results support our previous discussion, highlighting two key findings. First, the combined effects of RT and BTX are superior to either sole intervention, as demonstrated by the results of Group B0R0 from W0 to W4. Group B0R0, which exhibited significant improvements in STward-in but not in NTward-out, suggests that the combination of BTX and RT can enhance upper limb function in individuals with post-stroke upper limb spasticity, albeit with a more limited impact on relatively less challenging tasks. For individuals in the acute or subacute phase of stroke, when neuroplasticity remains highly active, these effects may influence the recovery trajectory, particularly given the established benefits of early BTX injection [36]. Therefore, early interventions, as seen in Group B0R0, may be advantageous during the initial phase after stroke.
Second, the training effects of RT were most pronounced when spasticity was maximally reduced due to BTX injection, as observed in Group B0R4 from W0 to W8. Group B0R4 showed significant improvements in both NTward-out and STward-in, with NTward-out being the more challenging task. The results from W0 to W8 further suggest that more complex tasks require more time to achieve significant improvements than simpler tasks. This can be understood in the context of BTX creating a plastic state, enabling subsequent RT to drive functional improvements through motor learning, a process that requires time. This interpretation is supported by the fact that NTward-out movements demand greater strengthening of agonist muscles and improved coordination, in addition to spasticity reduction, compared to STward-in movements.
These findings suggest that Group B0R4 exhibited more fundamental improvements in motor function, representing the most effective approach. Therefore, for individuals with chronic stroke who have limited access to resources, an approach in which RT begins when BTX effects are maximized, starting RT approximately 2 weeks after BTX injection, would be preferable, considering the mode of action of BTX. Although Group B0R4 was designed to initiate RT 4 weeks post-BTX for study robustness, these findings suggest that earlier RT initiation may optimize rehabilitation outcomes.
Study limitations
There are several limitations to this study. First, we enrolled only individuals with chronic stroke, which limited our ability to observe the effects of BTX and RT in the subacute phase, where natural recovery processes may be more prominent. Given the potential for neuroplasticity and the impact of earlier rehabilitation and BTX administration in the early phase of stroke, results from subacute phase individuals with stroke might be more pronounced than the current findings [36, 37]. The delayed initiation of RT in individuals with chronic stroke may have limited the degree of neuroplastic adaptation, whereas earlier intervention in the subacute phase could potentially enhance synaptic remodeling and motor learning. Future studies should explore whether initiating RT at the peak of BTX efficacy in the subacute phase produces greater functional gains. Second, the sample size was small. Additionally, a power analysis to determine the required sample size was not performed, as this study was designed as a pilot investigation. However, we used kinematic data, which is more sensitive than clinical scales, allowing us to capture significant findings despite the small sample size. Third, spasticity in muscles other than the elbow flexors was not treated with BTX injection, which may limit the generalizability of the results to all individuals with ULS. Fourth, participants received conventional therapy in addition to the study interventions, which may have influenced the results, particularly the effects of RT. However, given that all participants received the same amount of intervention, we believe our results primarily reflect the effects of RT and BTX.
Therefore, further studies with a larger sample size and sufficient statistical power based on the present study’s findings are needed. Additionally, studies that include individuals in the subacute phase of stroke who may have greater potential for neuroplasticity are warranted.




Comments (0)