
Remember me


This study was approved by the Certified Review Board (CRB3200011) of the National Center for Global Health and Medicine and registered as a specific clinical study (jRCTs032220082) in the Japan Registry of Clinical Trials. We included patients aged ≥20 years with American Society of Anesthesiologists’ physical status (PS) I–III; without significant cardiovascular comorbidities; scheduled for elective surgery under total intravenous anesthesia (TIVA) with propofol, remifentanil, and rocuronium; and who did not meet the exclusion criteria outlined in Table 1. Informed consent was obtained from all participants before assigning them via randomization into either the manual or automated control group. The study employed a single-center, single-blinded, randomized, parallel-group design, with only the patients blinded to group allocation.
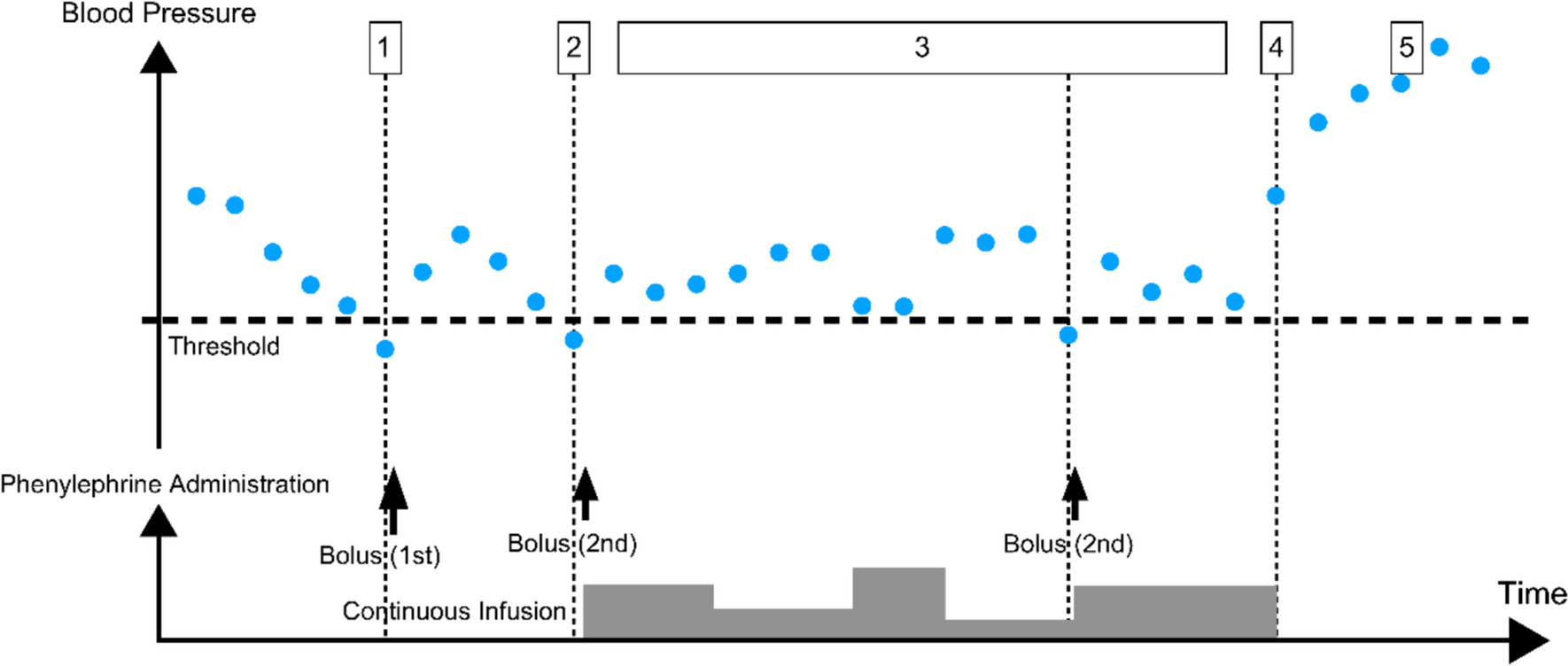
Table 1 Exclusion criteriaClinical application of the systemThe system developed in this study is a lower limit control system that administers phenylephrine when the measured mean blood pressure falls below a threshold value (Fig. 1). It does not set a target blood pressure value for each patient or administer vasopressors to maintain constant blood pressure as in previous reports [3, 4]. We used a model-free control as it is difficult to create a mathematical model to explain blood pressure fluctuations in patients in a clinical setting; even if one were created, the accuracy of the model could not be guaranteed. Since the objective of this system is lower limit control, a rule-based, closed-loop, data-driven control algorithm was implemented instead of classical methods, such as PID control. As this represents the first stage of development, the system lacks the capability to predict a drop in blood pressure several minutes after multiple measurements and to administer vasopressors prophylactically. Notably, the system was designed to assist anesthesiologists and other clinicians in hemodynamic management and was not intended to diagnose or treat the underlying cause of hypotension.
Fig. 1
Conceptual framework for automated phenylephrine administration. 1. Upon detection of mean blood pressure (MBP) falling below the predefined threshold, the system administers the first bolus of phenylephrine. 2. If MBP remains below the threshold, a second phenylephrine bolus is administered, followed by the initiation of continuous phenylephrine infusion. 3. The phenylephrine infusion rate is adjusted based on subsequent MBP readings. 4. Continuous phenylephrine administration is discontinued when MBP is sufficiently above the threshold. 5. The device remains inactive if MBP exceeds the upper safety limit
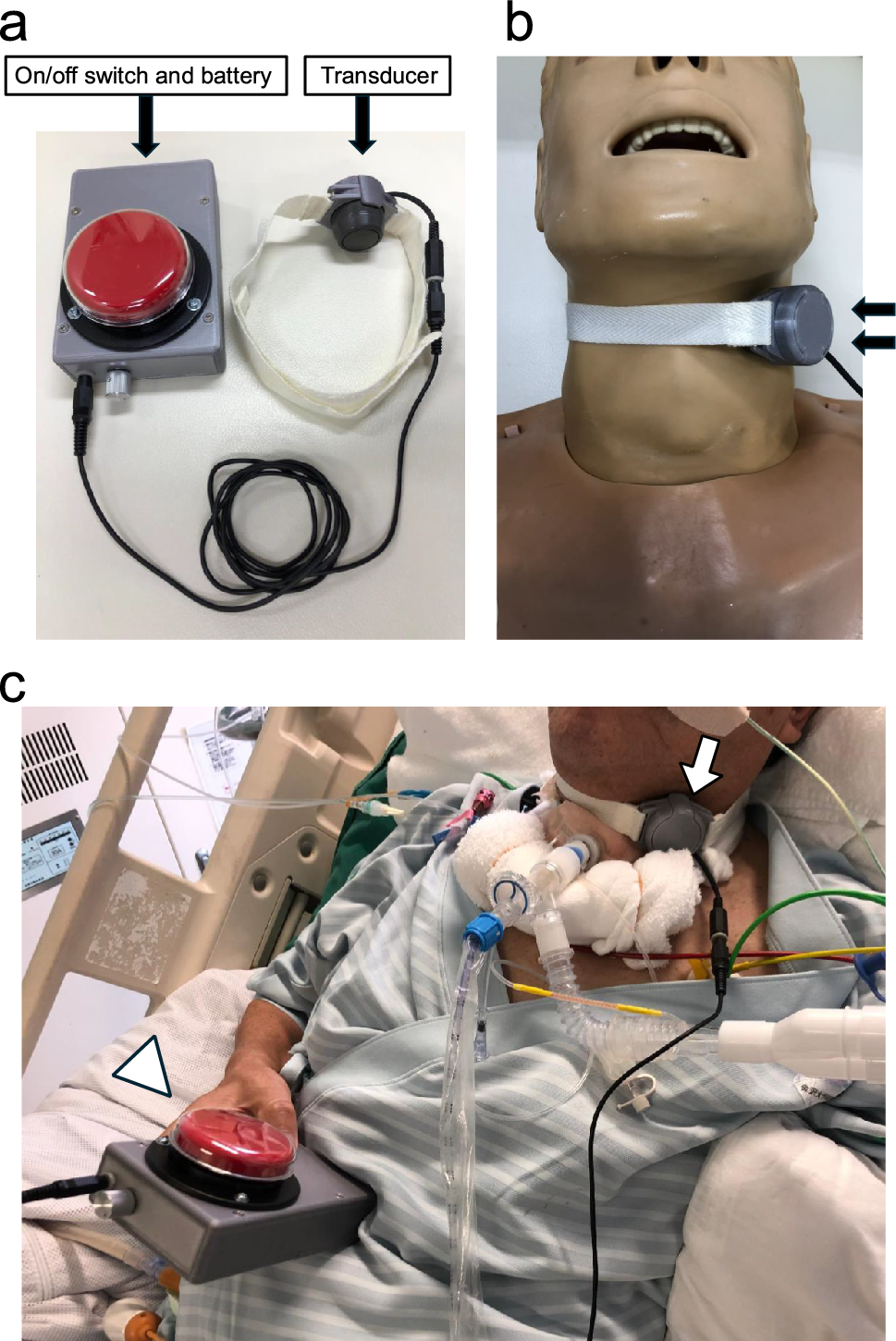
In this system (Fig. 2), information from the biometric monitor (BSM-6701/CSM-1701, Nihon Kohden Corporation, Tokyo, Japan) is provided via LAN to the control software running on a laptop computer with Windows 11 Professional, as in the anesthesia recording system. The control software calculates the phenylephrine dose using programmed rule-based calculations each time NIBP is measured at 2.5-min intervals. If the blood pressure cannot be measured due to a measurement error, the control state is not changed. If an abnormal value is measured, the dosage rate is calculated accordingly, and the dosage rate is also corrected at the next measurement, or a temporary re-measurement by the anesthesiologist. The calculation results are transferred to the syringe pump (TE-SS830, Terumo Corporation, Tokyo, Japan) through a communication rack (TE-RS800N, Terumo Corporation, Tokyo, Japan) via LAN, and the administration rate of phenylephrine solution (0.05 mg/mL) is changed. This control software was added to the automated delivery system for TIVA [5], which changes the dosing rate of three syringe pumps filled with propofol, remifentanil, and rocuronium solutions.
Fig. 2
The configuration of this system. LAN local area network, TIVA total intravenous anesthesia
Intraoperative patient managementWe utilized an automated delivery system for TIVA [5] to objectively standardize the administration of general anesthetics, including propofol, remifentanil, and rocuronium. We incorporated a function to automatically manage the dosage of vasopressors based on our original algorithm for this system and were able to eliminate the effects of the anesthesiologist's arbitrary decisions on the administration of anesthetics.
Upon admission to the operating room, an intravenous infusion circuit is connected to administer intravenous anesthetics and vasoactive drugs by securing the intravenous line (≥20G in diameter). Using an infusion pump (TE-LM835A, Terumo Corporation, Tokyo, Japan), 1% glucose-acetate Ringer's solution is administered at an initial rate of 10 mg/kg/h from the infusion circuit. The patient received 6 L/min of oxygen through a face mask, and a cuff for NIBP measurement was applied to the upper arm. Electrodes for muscle relaxation monitoring (NM-345Y, Nihon Kohden Corporation, Tokyo, Japan) were placed on the forearm and hand. An electrode for electroencephalogram measurement (BIS Quattro Sensor, Covidien Japan Corporation, Tokyo, Japan) was attached to the forehead to monitor bispectral index (BIS) values. An SpO2 adhesive sensor (TL-281T-1B, Nihon Kohden Co., Ltd., Tokyo, Japan) was placed on the fingertips for calibration, and the noninvasive estimated continuous cardiac output (esCCO) system [6] was used to measure circulatory parameters including estimated continuous cardiac index (esCCI) and estimated stroke volume index (esSVI). After adequate oxygenation and denitrogenation, continuous remifentanil administration was initiated using the automated delivery system for TIVA [5], followed by propofol administration, also controlled by the system. Following calibration of the muscle relaxation monitor after the patient was anesthetized, muscle relaxation with rocuronium was achieved, and tracheal intubation was performed. Depending on the progress of the surgery and the state of the anesthesia, the anesthesiologist changed the infusion rate of 1% glucose-containing acetic acid Ringer’s solution based on empirical rules while referring to fluctuations in blood pressure. In addition, antibiotics, single-dose drugs, and additional infusion products were administered through the side tubes of the infusion route as needed. Subsequent administration of propofol, remifentanil, and rocuronium was regulated by the automated delivery system for TIVA through closed-loop control, utilizing BIS values and train-of-four count as indicators [5].
Treatment of abnormal hypotensionIn this study, NIBP was measured every 2.5 min in all patients. MBP <65 mmHg was defined as abnormal hypotension, while SBP >140 mmHg was classified as hypertension.
In the manual group, when MBP indicated abnormal hypotension, phenylephrine was administered as a single injection of up to 0.1 mg or as a continuous infusion (maximum 2 mg/h) at the discretion of the anesthesiologist with board certification. Phenylephrine was initiated only after the onset of abnormal hypotension, and prophylactic administration in the absence of hypotension was prohibited.
In the automated group, the device automatically regulated phenylephrine administration according to the following algorithm (Fig. 1):
When MBP is abnormally low, the control device enters vasopressor administration mode, administering an initial dose of 0.002 mg/kg of phenylephrine (maximum 0.1 mg). If hypotension persists, an additional dose of half the initial amount is administered, followed by a continuous infusion at a rate determined by the protocol.
If the anesthesiologist determined that automated administration was insufficient to raise the pressure, a manual dose of phenylephrine was administered and recorded along with the time.
If MBP recovers from hypotension, continuous phenylephrine administration is maintained or resumed at the protocol-determined dosing rate if MBP is < 85 mmHg. If MBP exceeds 85 mmHg, continuous administration is suspended, following protocol calculations.
If continuous phenylephrine administration is interrupted for > 15 min, the system exits vasopressor administration mode and returns to normal.
If the anesthesiologist judged that the patient could not recover from hypotension with continuous phenylephrine administration, the initiation of continuous noradrenaline administration was considered.
Statistical analysisThe evaluation period for statistical analysis spanned from the initiation of remifentanil to the completion of propofol/remifentanil administration. The full analysis set (FAS), which represents the maximum analysis population, included patients who did not receive phenylephrine and experienced no episodes of abnormal hypotension during the evaluation period. These patients were considered to be in an unusually favorable regulatory situation, with an abnormal hypotension time rate of 0, despite no interventions being made to avoid hypotension. Consequently, these patients were excluded from the protocol per set (PPS). Patients who required continuous noradrenaline administration were also excluded from PPS. Missing NIBP values were left as missing and not included in the evaluation period.
The primary end point, the adequate blood pressure time percentage, was defined as the percentage of time during the evaluation period when MBP >65 mmHg and SBP <140 mmHg were maintained. This value was calculated by subtracting the percentage of time during the evaluation period when either abnormal hypotension (MBP <65 mmHg) or hypertension (SBP >140 mmHg) occurred. The non-inferiority of the automated group compared to that of the manual group was assessed using a t test with a non-inferiority margin of 10% and a significance level of 5%.
Secondary end points included the percentage of cases requiring vasopressors other than phenylephrine, use of additional vasopressors administered by the anesthesiologist, total dose of phenylephrine and infusions, percentage of time with adequate anesthesia from the start to the end of surgery, esCCI, esSVI, and MBP variability.
For safety evaluation, adverse events occurring from the day of surgery until 48 h postoperatively were assessed. Adverse events were evaluated based on the date of onset, event name, severity, treatment, outcome, and the causal relationship to the study. They were categorized as adverse events observed in subjects, adverse events observed in non-subjects, and study equipment malfunctions.
Sample size designDue to the absence of previous or similar studies, we assumed that the regulatory performance would be comparable between the manual and automated groups, as described in a developmental study of the automated delivery system for TIVA [7]. We calculated a power of 90%, a non-inferiority margin of 10%, and a dropout rate of 20% (e.g., no circulatory agonist administered). The required sample size was calculated to be 20 patients in total.
Comments (0)