
Remember me


This study was conducted and reported in accordance with the Strengthening the Reporting of Observational Studies in Epidemiology (STROBE) statement. This retrospective, single-center, descriptive study investigated the period from 1 April 2019 to 30 June 2024 at Aichi Children’s Health and Medical Center, a tertiary-care hospital in Japan. This study was approved by the institutional ethics committee (approval no. 2024023; date of approval: 1 July 2024). The requirement for written consent was waived by the institutional ethics committee based on the retrospective nature of this study.
Inclusion and exclusion criteriaThis study included patients ≤ 3 years old with dimples identified immediately prior to caudal epidural block, who were scheduled to undergo their first urological surgeries during the study period. In the absence of preoperative s-MRI, s-US was performed just before the caudal epidural block to evaluate for underlying TCS. Enrolled patients were categorized into two groups: (1) Group T, in which spinal abnormalities potentially causing TCS were detected on postoperative s-MRI; and (2) Group N, which included cases where no spinal abnormalities were identified on s-US or where abnormalities were suspected on s-US but not confirmed on postoperative MRI. The indications for caudal epidural block included urethroplasty for hypospadias, orchidopexy for cryptorchidism, ureterocystoneostomy for vesicoureteral reflux, renal pelvis reconstruction surgery for hydronephrosis, and endoscopic urethrotomy for urethral stricture.
The exclusion criteria were as follows: (1) patients who had previously undergone spinal surgeries before first urological surgery; (2) patients who had not undergone postoperative s-MRI when s-US detected spinal abnormalities.
Systematic spinal ultrasound screening (convenient conus to coccyx point-of-care ultrasound)At our institution, s-US serves as the standard procedure for detecting TCS during the evaluation of patients with dimples. We performed s-US using the previously reported method [2]. Even if ossification of the vertebral posterior arch is present, structures within the spinal canal and sacral canal can be observed using spinal ultrasound through the lumbar intervertebral spaces and sacrum as shown in Fig. 1. We conducted caudal epidural block in cases where no TCS were detected. All s-US was performed with the patient in a lateral decubitus position after completing the induction of general anesthesia. First, utilizing the lowest rib (the 12th thoracic vertebra: T12) as a reference point, we systematically acquired continuous horizontal ultrasound images of the spinal cord extending from T12 to the coccyx using a sliding ultrasound probe. Second, we assessed the sacral canal in the sagittal plane. The current method can determine the following: (1) the lowest point of the conus medullaris (usually situated cranial to L2 in normal anatomy); (2) the lowest point of the dural sac (typically cranial to S2 in normal anatomy); (3) the width of the filum terminale, using a value < 1.1 mm for differentiation from filum terminale lipoma; and (4) the presence of cysts and lipomas in the sacral canal. We utilized HSL25x® ultrasonography kits (6–13 MHz, linear; FUJIFILM Sonosite, Bothell, WA, USA). The quality of spinal ultrasonography was ensured by having trained pediatric anesthesiologists perform the procedure. A senior anesthesiologist received training in s-US from pediatric radiologists. Pediatric anesthesiologists who had undergone more than five on-the-job training sessions with the senior anesthesiologist performed the spinal ultrasound. In addition, the senior anesthesiologist reviewed all spinal ultrasound images either during the procedure or on the same day the procedure was performed.
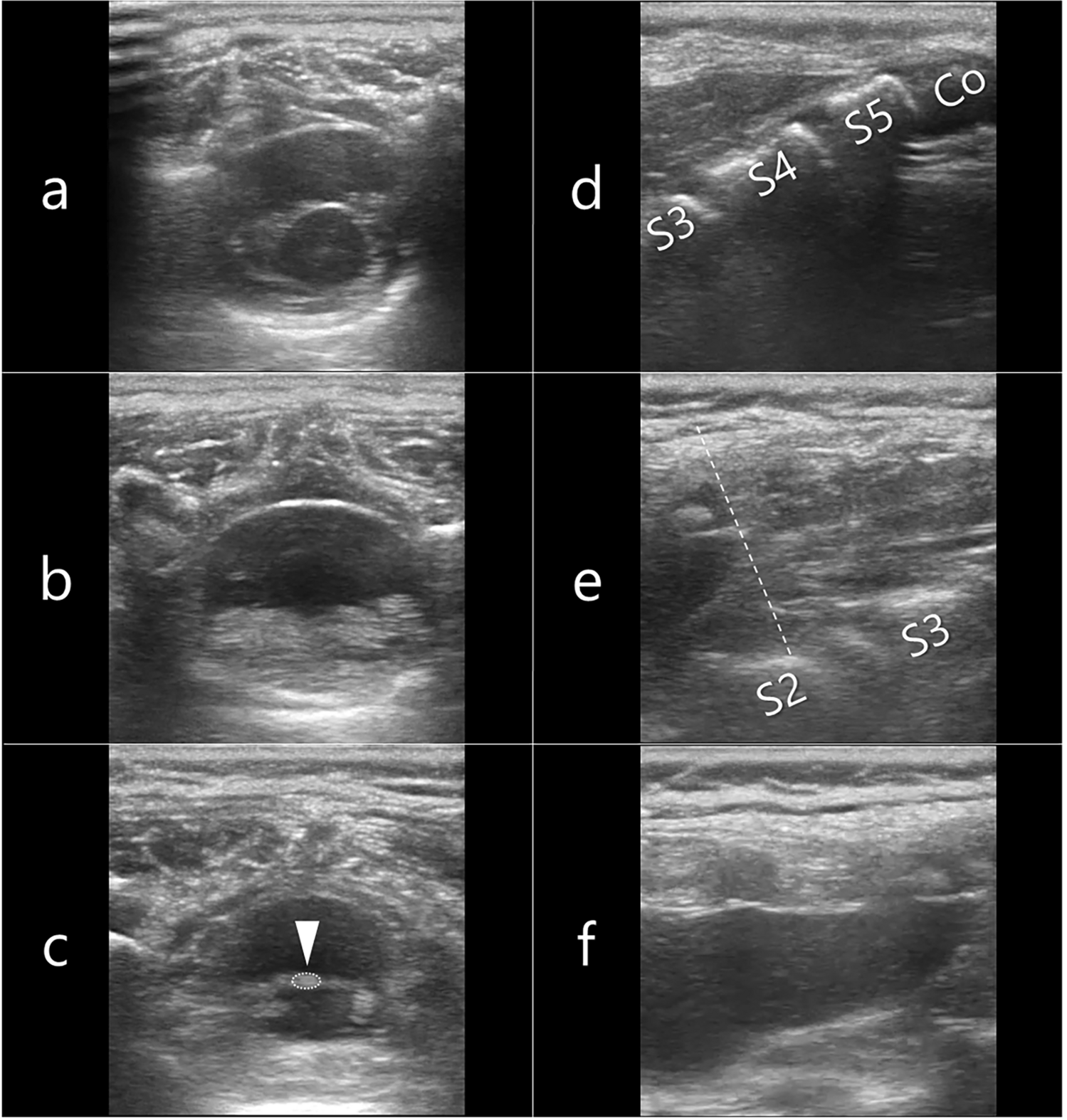
Fig. 1
Key imaging findings from systematic spinal ultrasound screenings of a 16-month-old child. a Horizontal image between T12 and L1, showing the conus medullaris and cauda equina. b Horizontal image between L2 and L3, predominantly displaying the cauda equina within the dural sac, as the conus medullaris typically terminates at the L2 level. c Horizontal image between L5 and S1, where the filum terminale (arrow) can be identified due to dispersion of the cauda equina. d Sagittal image on which the sacral level can be determined by the position of the coccyx. e Sagittal image on which the structure in the sacral canal can be assessed, and the end of the dural sac (dotted line) can be identified. f Sagittal image showing structures within the dural sac, including the filum terminale. Co coccyx, S sacrum
Spinal magnetic resonance imagingFor postoperative s-MRI, a 1.5-T system (Ingenia; Philips Medical Systems, Best, the Netherlands) was used, with T1- and T2-weighted images in both short- and long-axis views employed to diagnose TCS. Consultation with a neurosurgeon was conducted by pediatric urologists to assess the risk of future neurogenic bladder development based on patient characteristics in cases where TCS was suspected from s-US findings and dimple morphology. The neurosurgeons performed postoperative s-MRI, referencing the s-US images shared in the electronic medical records. Imaging parameters for T1-weighted s-MRI were as follows: repetition time, 475 ms; echo time, 11 ms; flip angle, 90°; section thickness, 5 mm; matrix size, 288 × 169; and field of view, 180 mm. The imaging parameters for T2-weighted s-MRI were: repetition time, 4,439 ms; echo time, 120 ms; flip angle, 90°; section thickness, 5 mm; matrix size, 288 × 104; and field of view, 180 mm. Neurosurgeons reviewed the MRI findings and diagnosed filum terminale lipoma if the filum terminale showed signal hyperintensity on axial T1-weighted images.
Data collectionDemographic data recorded from electronic medical records included age, sex, height, body weight, diagnosed urological diseases, gestational age, and birth weight. We assessed the risk of potential TCS by measuring the size of the dimple and its distance from the anus as part of standard care, and we recorded this information in the anesthesia records for communication with neurosurgeons and urologists. Dimple size and dimple-anus distance were measured after positioning the patient in the left lateral decubitus position for caudal epidural block, using a flexible paper ruler that conforms to the curvature of the gluteal region. Information regarding dimples was collected from anesthesia records, including: (1) short and long diameters of the dimple; and (2) dimple-anus distance. The dimple was predominantly elongated along the cephalocaudal axis, with the longitudinal extent along this axis constituting the long diameter, and the transverse extent (from left to right) constituting the short diameter.
Collection and analysis of data derived from spinal ultrasound screening and spinal magnetic resonance imagingIn this study, we recorded key anatomical landmarks, including the lowest points of the conus medullaris and dural sac, as well as measurement of the filum terminale obtained from both s-US and s-MRI. In addition, we recorded the specific spinal diseases diagnosed from s-US and s-MRI. A filum terminale thickness ≥ 1.1 mm was considered as filum terminale thickening [7]. The minimum filum terminale thickness was defined as 0.1 mm, corresponding to the limit of detection for the ultrasound device employed. We tried to describe the optimal cutoff value for filum terminale thickness measured by s-US in detecting filum terminale lipoma, as conclusively diagnosed by s-MRI.
Adverse events related to caudal epidural blockRopivacaine was administered for caudal epidural block at a maximum dose of 3 mg/kg, diluted to concentrations ranging from 0.25 to 0.1875%. Adverse events of caudal epidural block such as local anesthetic toxicity, cerebrospinal fluid aspiration, lower limb motor impairment, and sensory disturbances, were extracted from medical and anesthesia charts.
Proportion of cases in which spinal surgery was performedWe described the proportion of cases in which spinal surgery for TCS was performed based on the results of s-US and s-MRI.
Sacral dimple morphologyWe described the number of cases in Groups T and N with: (a) long diameter of the dimple ≥ 5 mm; and (b) dimple–anus distance ≥ 25 mm [6].
Filum terminale thicknessWe described the number of cases in Groups T and N with filum terminale thickness ≥ 1.1 mm [7]. In addition, we tried to determine the optimal cutoff value for filum terminale thickness as measured by s-US for detecting filum terminale lipoma.
Statistical analysisThe patient demographics and clinical characteristics were compared between Groups T and N. The outcome measures are presented as median with interquartile range (IQR) or as count and percentage. The Mann–Whitney U-test was utilized to assess continuous variables with skewed distributions, while the χ2 test or Fisher’s exact test was used for comparing categorical variables to assess differences in patient characteristics between groups. The following cutoff values were assessed using the χ2 test: (a) long diameter of the dimple ≥ 5 mm; and (b) dimple-anus distance ≥ 25 mm. We used the receiver operating characteristic (ROC) curve to determine the optimal cutoff value for filum terminale thickness measured by s-US in detecting filum terminale lipoma, as conclusively diagnosed by s-MRI. Youden’s index is used to identify the value that offers maximal sensitivity and specificity on the ROC curve [8]. We calculated Youden’s index to determine the optimal cut-off for detecting spinal abnormalities from s-US. Patients with missing values were excluded. Data were analyzed utilizing STATA 17.0 (StataCorp, College Station, TX, USA), with a two-sided p value < 0.05 indicating statistical significance.
Comments (0)