
Remember me


After approval of the local ethical committee (IRB 00006379//31-1-2022), this study was registered prior to patient enrollment at ClinicalTrials.gov (NCT05218733) and adhered to standards of the Helsinki Declaration 2013. This clinical trial was performed between February 15, 2022 and September 20, 2023 at Ain-Shams University Maternity Hospital. Each patient signed a written informed consent before the operation.
Study populationThis clinical trial was conducted on 120 females, aged 40–55 years, body mass index (BMI) < 35 kg/m2, American Society of Anesthesiologists (ASA) I, II physical status, and listed for elective open TAH via Pfannenstiel incision under GA. Patients with hepatic or renal dysfunction, severe cardiovascular disease, coagulopathy, pulmonary function compromise, obstructive sleep apnea, diabetes mellitus or prediabetes, and pre-existing chronic pain were excluded. Patient’s refusal, local infection at site of block, known allergy to study drugs (bupivacaine or morphine), altered mental status and pre-existing steroid treatment were also causes of exclusion from this study.
Randomization and blindingAfter randomization using computer-generated random numbers kept in sealed opaque envelopes and based on PO pain management protocol with an allocation ratio of 1:1:1, patients were allocated to the ESPB group, ITM group or control group. An anesthesiology resident picked the envelope to know the patient`s assigned group. All patients received GA. By the end of surgery and before extubation, patients in the ESPB group obtained bilateral US-guided ESPB and sham block at the lumbar puncture site; patients in the ITM group obtained 0.3 mg of preservative-free morphine dissolved in 3 mL normal saline (NS) intrathecally and bilateral US-guided sham block at the ESPB puncture sites and patients in the control group obtained a bilateral US-guided sham block at the ESPB puncture sites and a sham block at the lumbar puncture site. Both the ESPB and ITM groups were the intervention groups. US-guided ESPB was performed by experienced anesthesiologists who had no additional role in this clinical investigation. Every sham block was conducted using 2 mL NS solution of a subcutaneous injection at the corresponding block site. Anesthesiology residents, blinded to patient allocation, evaluated and recorded the clinical trial outcomes. The procedures were performed by the same experienced gynecologic surgeons’ team. Patients and surgeons were also blinded to allocation of treatment groups.
Study non-dependent protocolFollowing the fulfillment of routine preoperative evaluation, patients were taught about the visual analog scale (VAS) (0–10 cm) to rate nausea and pain at rest and with cough [12]. Nausea was rated from 0 = no nausea to 10 = the worst nausea imaginable, and pain was rated from 0 = no pain to 10 = the worst pain imaginable. Patients received 150 mg ranitidine tablet the night before surgery and abstained from solid food for 6 h prior to surgery. Patients were also premedicated with 3 mg IV granisetron, and antibiotic prophylaxis after establishment of an intravenous (IV) line. A baseline reading of vital data was obtained for every patient after applying the standard operating room monitors.
Induction of GA was established with fentanyl 1.5 µg/kg and propofol 1.5 mg/kg, followed by rocuronium 0.6 mg/kg to facilitate orotracheal intubation. Following intubation, a Foley catheter was inserted for measurement of urine output and remained in place for 24 h. Anesthesia was maintained with 1–1.5% isoflurane with 50% oxygen in air and a top-up of muscle relaxant was provided on demand. All patients were mechanically ventilated to keep the EtCO2 between 35 and 40 mmHg. Additional boluses of fentanyl (0.5 ug/kg) were given if heart rate (HR) or mean arterial pressure (MAP) increased more than 20% from baseline values and the total intraoperative fentanyl doses were documented. 1 g IV acetaminophen was administered for all patients 15 min before the end of surgery and every 6 h till 24 h following surgery. By the end of surgery, every patient was laterally positioned and underwent an ESPB, spinal anesthesia or sham block according to the patient`s group allocation, followed by placing in the supine position again. The inhalational anesthetic was turned off and the residual neuromuscular paralysis was reversed by neostigmine (0.05 mg/kg) and atropine (0.01 mg/kg). After extubation, every patient was sent to the post-anesthesia care unit (PACU). The hemodynamic variables (HR and MAP) of patients were documented at T0: before induction of GA; T1: mean intraoperative changes of both HR and MBP before the procedure (ESPB, ITM or sham block); T2: 20 min after performing the block; T3, T4, T5, T6 and T7 which matched 2, 6, 12, 18 and 24 h postsurgery, respectively. VAS pain scores at rest and on coughing were assessed at 30 min, 2, 6, 12, 18 and 24 h after surgery. The PO level of sedation of every patient was appraised using the Richmond Agitation Sedation Scale (RASS) [13]. Patients were transferred to the gynecology ward when they got a modified Aldrete score ≥ 9.
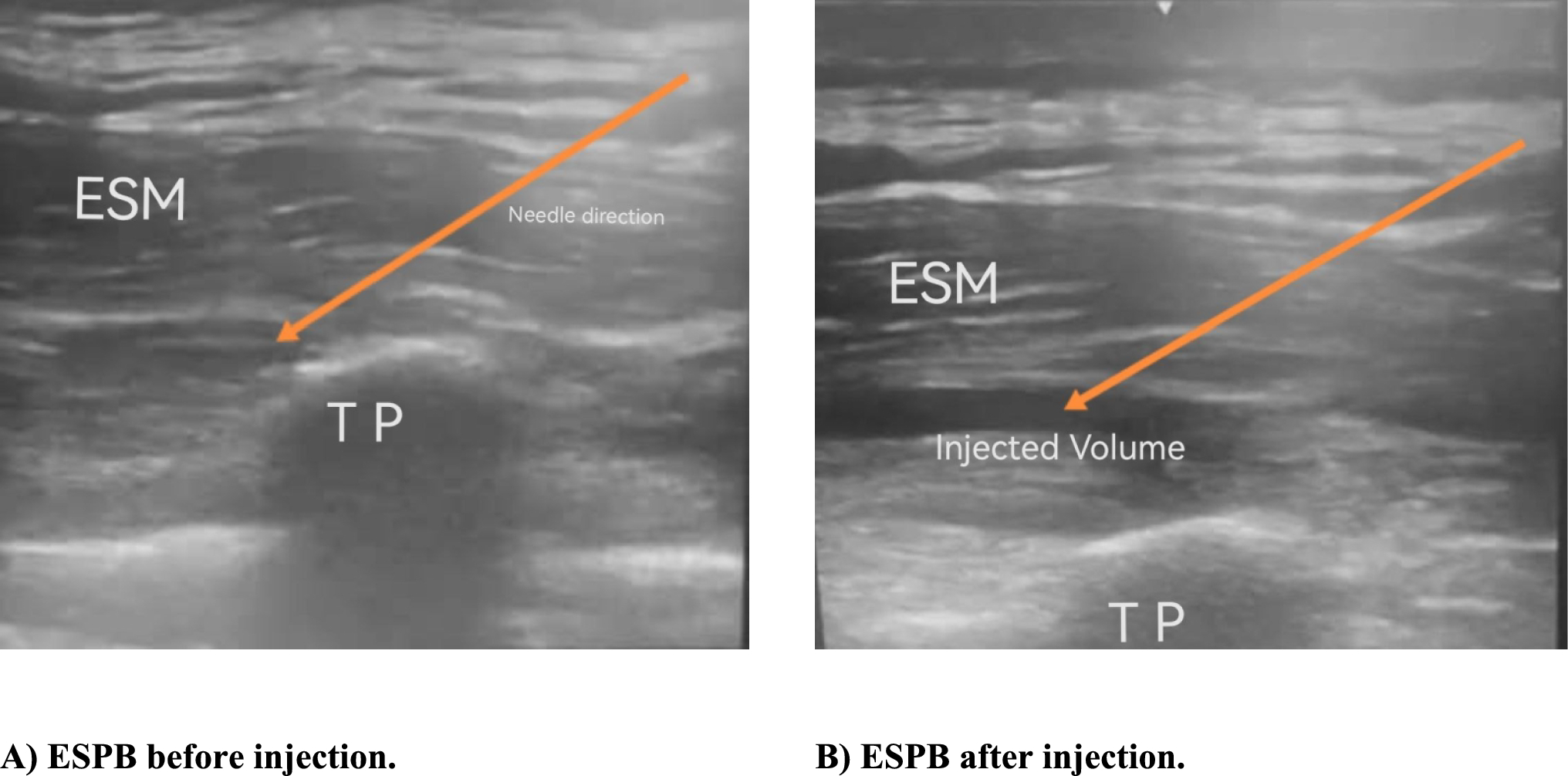
Study-dependent protocolUS-guided ESPB techniqueAfter skin sterilization with povidone-iodine solution, ESPB was achieved at the level of the spine of the ninth thoracic vertebra (T9). T9 was located by counting down from the spine of the seventh cervical vertebra. A high-frequency (5–13 MHz) linear US transducer (M‑turbo; Fujifilm SonoSite Inc., Bothell, Washington, USA) was placed vertically 3 cm lateral to the T9 spinous process. An 80 mm 22-gauge block needle (Stimuplex® D, B-Braun, Germany) was placed using an in-plane approach. The needle tip was inserted into the fascial plane on the deep aspect of the erector spinae muscle (ESM). The correct location of the needle tip was verified by 2–3 ml of NS injectant for hydrodissection of the interfascial plane between the ESM and the transverse process. A total volume of 20 mL of 0.25% bupivacaine was injected through the needle. The same technique was repeated on the opposite side (Fig. 1).
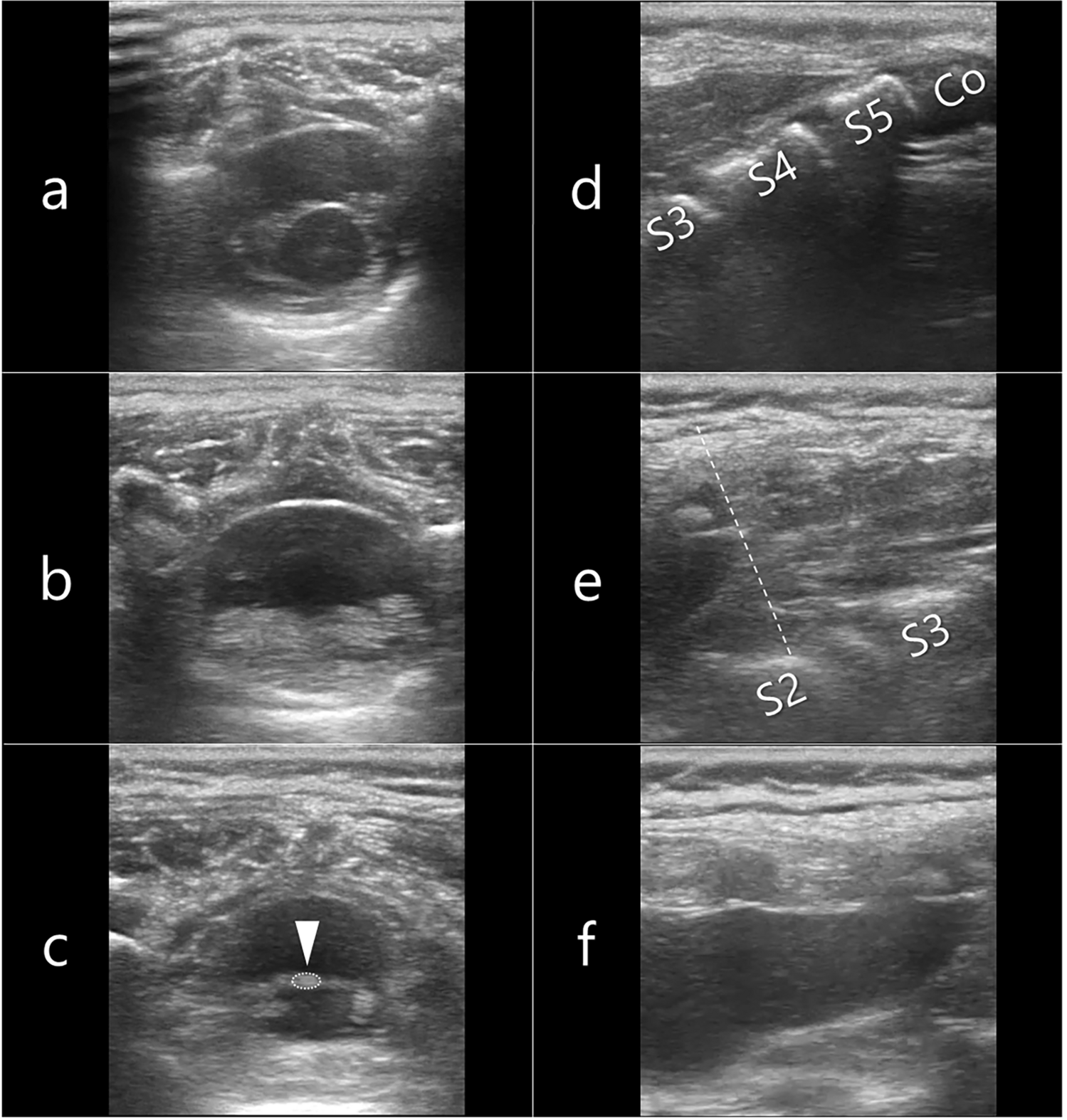
Fig. 1
US pictures demonstrating the direction of the needle and anatomical landmarks during ESPB. [(A) ESPB before injection, (B) ESPB after injection)] (ESM erector spinae muscle, ESPB erector spinae plane block, TP transverse process, US ultrasound)
ITM groupMorphine (10 mg/mL) was added to 100 ml saline dilution bag to achieve a concentration of 100 μgm/mL. The anesthesiologist assigned to perform the intrathecal injection drew 3 ml from the dilution bag in a 3 ml syringe. After skin sterilization with povidone-iodine solution, the dura was punctured at the L4–L5 or L5–S1 intervertebral space using a 25G Quincke spinal needle and the prepared 3 ml diluted morphine (0.3 mg) injected after confirming free flow of the CSF through the needle.
Parameters and outcomesHR and MAP were listed at different time points during the study. The time to perform the regional anesthesia technique was documented. All patients were treated with a rescue analgesia of 100 mg tramadol (ampoule) diluted in 100 ml of NS. This rescue dose was infused over 15 min for a VAS > 3 or patient`s request for analgesia and not exceeding 400 mg/day. The time to first request for a rescue analgesic and the total tramadol consumption/24 h after surgery were reported. Admitting more than one dose of rescue analgesic medication to the patient in the first hour after surgery was considered as a failed block which was recorded and omitted from the study results.
Recovery parameters including the length of PACU stay (min), time to unassisted ambulation (h), time to return of gastrointestinal function (passing flatus) (days) and hospital length of stay (LOS) (days) were listed.
The intervention related side effects including bradycardia, hypotension, PONV, pruritis, RD (respiratory rate < 12 breaths/min), LA toxicity and block technique adverse events (local site infection, hematoma formation and pneumothorax) were assessed. If patient experienced nausea at a VAS score > 7 or one emetic episode, she received 10 mg IV metoclopramide. Pruritus was appraised using a four-point scale [13] and patient with severe pruritus was treated with 45.5 mg IV pheniramine maleate (AvilR). Sedation, respiratory rate and oxygen saturation (SpO2) were monitored for 24 h after surgery. 0.4 mg IV naloxone was administered and supplemental oxygen by nasal cannula at 6 l/min if the patient had SpO2 ≤ 94% or RASS of − 4, or − 5. Patient satisfaction with PO pain control regimen was recorded at 24 h after surgery using a five-point Likert scale [14].
Laboratory analysisThree samples (3 mL each) of venous blood were collected from each patient included in this study under complete aseptic conditions; one hour before the operation as a baseline sample (8 a.m.) (H0), 2 h after the operation (H1) and 24 h postoperatively (H2) for assessment of serum glucose and serum cortisol. The blood was left to clot for 30 min in sterile dry vacutainers. The serum was then separated by centrifugation at 3500 rpm for 15 min, for the immediate assessment of serum glucose and serum cortisol. The analysis was done on COBAS e 402 and COBAS e 801 systems respectively supplied by Roche Diagnostics (GmbH, Sandhofer Strasse 116, D-68305 Mannheim).
The time to first rescue analgesic was the primary outcome measure of this study. Secondary outcome measures were VAS scores at rest and on coughing, the total tramadol consumption/24 h, hospital LOS, measurements of both serum glucose levels and morning serum cortisol levels, study-related adverse events and patient satisfaction.
Statistical analysisPower of the studyThe results from a prior pilot study, conducted by our research team, showed that the time to first rescue analgesia in the ESPB, ITM and control groups was 19.7 ± 1.5, 21.0 ± 1.6 and 0.8 ± 0.2 h, respectively, setting the power at 80%, alpha error at 0.017 for the three groups’ comparisons [15]. Depending on PASS 11th release program for sample size calculation [16], a minimal sample size of 32 patients/group was required to get a statistically significant difference based on the minimum difference among groups. We recruited 40 patients/group for possible dropouts and to study other secondary outcomes.
Data analysisStatistical Package for Social Sciences software version 28.0, IBM Corp., Chicago, USA, 2021, was used for data analysis. Qualitative variables were expressed as number and percentage and compared using Chi-square test as well as Fisher’s exact test for variables with small expected numbers. Quantitative variables were tested for normality using Shapiro–Wilk test, then expressed as mean ± standard deviation (SD) if normally distributed and compared using ANOVA (comparison between groups) and RMANOVA (comparison within groups) tests. If quantitative variables were not normally distributed, they were expressed as median (1st–3rd interquartile range) and compared using Kruskal–Wallis test (comparison between groups). Post hoc comparisons were done using Bonferroni test (comparison between groups, so homogenous groups had the same symbol “a, b or c”) and Dunnett’s test (comparison within groups, so times significantly different from T0 or H0 had symbol “⌂”). A p value < 0.050 was considered statistically significant.
Comments (0)