The results of the present study show that ID Migraine is a valid diagnostic tool even in children and adolescents. In both in children and adolescents, the ID Migraine showed an excellent profile in terms of sensitivity (85% and 87%, respectively), specificity (97% and 92%, respectively) and PPV (99% and 97%, respectively).
The diagnosis of migraine in pediatric age is often challenging. The ICHD 3 criteria are designed primarily for adults and may not fully account for the peculiarities of pediatric migraine [24]. The unique ways in which children experience and express migraine symptoms, combined with the variability in presentation, require careful consideration. Children may not fully understand or communicate their symptoms, making them dependent on caregivers to interpret and report their experiences. This can lead to underreporting or misinterpretation of the severity and frequency of symptoms. Young children may have trouble describing their pain, aura, or associated symptoms [24, 32]. Children may not meet all the ICHD 3 criteria for migraine diagnosis [25, 29, 33,34,35,36,37,38,39] and a consensus of pediatric headache experts proposes some recommendations in order to make criteria more appropriate for children [24].
Pediatric migraine attacks tend to be shorter in duration than those in adults. Migraine episodes in children may last as short as 2 h, making it harder to fit them into traditional diagnostic criteria, which typically require headaches to last 2 h or longer [4, 25, 29, 40]. Unlike adults, children may not always experience typical migraine symptoms such as a unilateral throbbing headache. Bilateral and less severe pediatric pain can lead to underdiagnosis or misdiagnosis [34].
In childhood and adolescence, determining a definitive diagnosis of primary headache can be hindered also by the change in headache type. According to report, 8–32% of migraine sufferers transition to TTH, and 4–41% of TTH sufferers’ transition to migraine [41]. There are two possibilities to explain the observed changes of childhood headache patterns. First, the 'continuum severity theory' states that primary headache is a continuum between TTH and migraine. In this model, headache is labelled tension-type when the pain is mild, as common migraine when the pain is more severe, and as classic migraine when the pain is associated with neurological symptoms [42]. Secondly, it is possible for children to experience two or more primary headache types that begin at different ages [25]. For this reason, in an attempt to test ID migraine in our population, we excluded patients diagnosed with TTH.
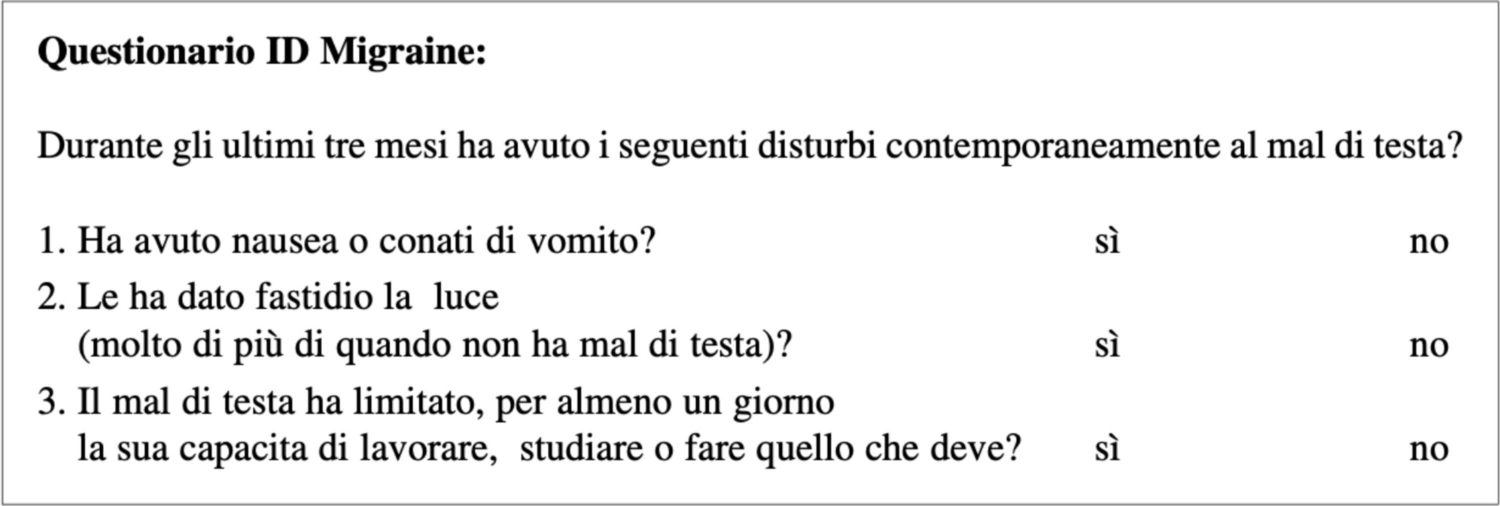
ID migraine tries to diagnose migraine based on the presence of photophobia, nausea, and pain- related disability. The questionnaire could also be adapted to pediatric age as these characteristics are frequently reported in children and adolescents with migraine. As our data also shows, the presence of these features provides ID migraine a valid tool despite the age of administration. In fact, in our sample in both age-related subgroups, ID migraine showed an excellent reliability profile despite the mean age of the two groups being different (8.58 years versus 14.75 years).
A previous study, conducted on patients under the age of 18 and suffering from migraine, found that most patients (83.4%) experienced at least one associated symptom between photophobia (79.2%) or nausea (64.5%) [40]. Another study showed that the best diagnostic items for migraine in children and adolescents are: 1) moderate or severe intensity, 2) pain aggravation by physical activity, and 3) pulsating quality of pain. Conversely, absence of photophobia or nausea, or no aggravation by physical activity were the most significant items in favor of TTH diagnosis [43]. In our sample photophobia was described by more than 60% of migraineurs, with a high specificity and PPV (81% and 94%, respectively). Nausea and vomiting were reported by 63% of migraine patients, while disability by 89%, thus supporting high reliability of ID Migraine (specificity 88% and 76%, PPV 95% and 94%). The presence of photophobia and phonophobia is less frequently described in pre-school children [25]. This could represent a problem for a possible ID migraine application to younger children. In the present study 73% of migraine patients reported photophobia, but children under 6 years were excluded from our observation.
Two previous studies investigated the validity of ID Migraine in pediatric age and their results disagreed (Table 3). Jin et al. achieved a specificity of 46.63% and a sensitivity of 39.71% investigated students aged from 7 to 15 years in a school context. The study was conducted in four primary schools where subjects were asked to complete a four-step questionnaire. In the first step, demographic features were recorded, and the presence of headache was screened. In the second one, 54 items were used to characterize the type of headache in migraine, TTH, cluster headache, and other headaches. In the third step, headache disability was recorded, while the fourth step was ID Migraine. The diagnosis obtained was migraine in 44.85% of subjects, TTH in 29.18%, cluster headache in 6.22%, and other headaches in 19.74% [23]. Zarigoflu et al. obtained a specificity of 71.1%, and a sensitivity of 62.1% from a three-steps interview administered to 12–17 years adolescent students. In the first phase, they were asked to fill a questionnaire concerning presence of headache and sociodemographic features. The second phase consisted in a face-to-face interview with students who had experienced headache. Lastly, the third step was the ID Migraine administration [27]. There are two main reasons which could explain the difference between both studies and our present results. First, our decision not to include TTH may have improved the sensitivity and specificity of the test. Indeed, in our control group patients suffered from headaches with characteristics clearly distinguishable from migraine and TTH. Second, we administered the test in a third-level headache center, which limits the generalizability of our results. For this reason, it is desirable to extend the administration to more settings. The generalizability of the tool provides its applicability to be stronger, allowing for earlier diagnosis.
Table 3 Studies investigated the validity of ID Migraine in pediatric ageThe early diagnosis of migraine in pediatric age is crucial for several reasons: 1) it helps to manage symptoms effectively, 2) it improves child’s quality of life, and 3) it prevents potential long-term complications. The timely introduction of appropriate treatments is possible only after an early diagnosis. Effective management can reduce the frequency and intensity of the headache attacks, preventing them from disrupting the child’s daily life. Whether migraine is not properly diagnosed and treated, it can become more severe over time, thus leading to an increased risk of chronification and medication overuse. In addition, early diagnosis provides the opportunity for both children and their families to learn about migraine triggers, symptoms, and coping mechanisms [28, 29].



Comments (0)