In this study, we aimed to review a single-centre experience of S. aureus vertebral osteomyelitis and assess the efficacy and safety of flucloxacillin as oral follow-up treatment. Among 24 patients treated with flucloxacillin as oral follow-up, the clinical cure rate at 12 months was 83%, indicating that prolonged flucloxacillin treatment might achieve cure rates similar to those reported by Park et al. [15] and Bernard et al. [16]. Thus, in selected cases, flucloxacillin could be a potential option for oral follow-up in these infections.
Only scarce data are available on the outcome after oral flucloxacillin follow-up treatment for vertebral osteomyelitis. No relapses were detected in a clinical and pharmacokinetic evaluation of a combination of flucloxacillin and probenecid in 1980 [12]; however, only four patients with osteomyelitis were included in the investigation, and the published article did not contain any extractable patient details. Beronius et al. [17] presented a Swedish cohort consisting of 42 patients, of whom 24 (57%) had received flucloxacillin as oral treatment. In general, the intravenous treatment duration was shorter compared to the present study, whereas the oral follow-up was longer (median 10 days and 179 days, respectively). The only relapse detected was in a patient receiving seven months of dicloxacillin as follow-up. Two additional case reports (without relapses) were presented in a recent narrative review [9].
As cephalosporins share mechanisms of action with other beta-lactams, their effectiveness in intracellular or biofilm environments is not expected to differ. The bioavailability of oral cephalosporins is variable, and the group includes drugs with high bioavailability (e.g., 95% for cephalexin). Okunmura et al. reported an 87% success rate (n = 15) for oral follow-up with cephalexin after at least 3 weeks of intravenous treatment, with a median total treatment duration of 86 days [18]. In another retrospective cohort study, a successful outcome was reported in 86% (n = 29) of patients treated with intravenous beta-lactam antibiotics followed by oral first-generation cephalosporins or amoxicillin/clavulanate for a median duration of 55–80 days [19]. There was no significant difference when comparing this oral step-down to patients receiving intravenous beta-lactam antibiotics for the entire treatment duration. Furthermore, longer treatments were associated with relapse, indicating a selection bias where the more complex high-risk cases were treated longer. In the present study, outcomes were similar, but the treatment durations exceeded those recommended by the Swedish national guidelines. As one of the relapses occurred in one of the patients receiving more than six months of treatment while most patients receiving 12–16 weeks of treatment achieved clinical cure, it is possible that a similar selection bias impacts the treatment duration in the present study.
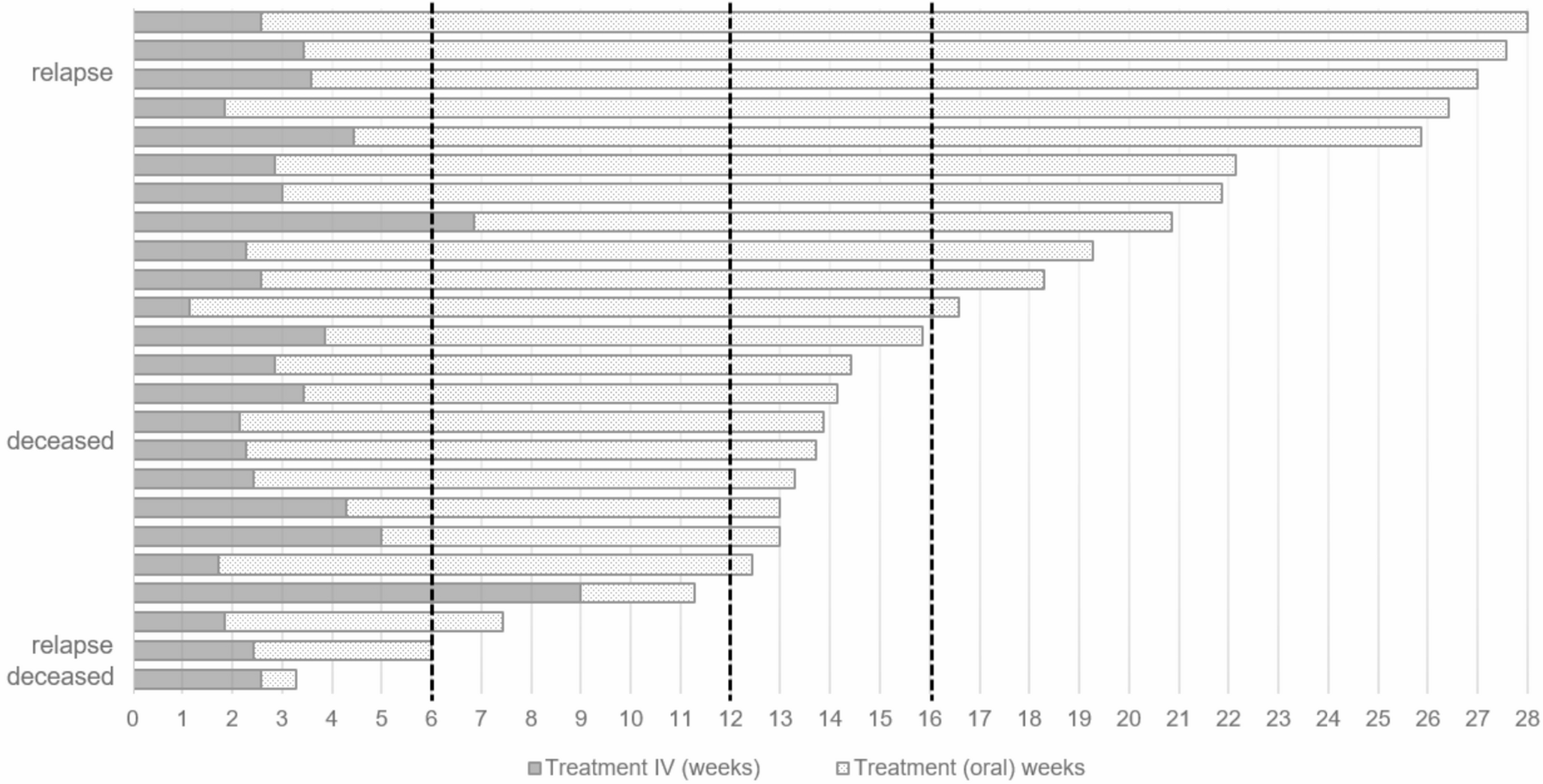
Bernard et al. [16] demonstrated that 6 weeks of antibiotic treatment was non-inferior to 12 weeks in vertebral osteomyelitis. However, the majority of patients received antibiotic combinations, mostly fluoroquinolone/rifampicin combinations (44%). Park et al. [15] identified methicillin-resistant S. aureus, undrained paravertebral/psoas abscesses, and end-stage renal disease as risk factors for relapse and recommended prolonged treatment (> 8 weeks) to these patients. It is notable that the studied populations were different, as the cohort studied by Bernard et al. included 19% abscesses, compared to 49% in the study by Park et al. [20]. In the present cohort, 72.5% of patients had an abscess, including 40% with paravertebral and/or psoas abscesses. One patient who relapsed after 6 weeks of treatment (including 4 weeks of flucloxacillin) had epidural and psoas abscesses, and was thus high-risk for relapse according to Park et al. Nevertheless, the optimal treatment duration for vertebral osteomyelitis when using flucloxacillin is unknown. In this cohort, the median treatment duration was 16.9 weeks, but five patients were treated for ≤ 13 weeks without relapse, even in the presence of abscesses. However, the above-cited data from oral cephalosporins [18, 19] suggest that 12 weeks could be sufficient for oral betalactam follow up treatment. However, considering the need for source control as well as the conditions for adequate antibiotic exposure is important when planning for oral follow-up.
The bioavailability and protein binding ability of flucloxacillin have led to concerns regarding its efficacy in complicated infections such as vertebral osteomyelitis. In a sub-study of the POET trial on oral treatment for infective endocarditis [21], the probability of target attainment (PTA) for the comparable oral drug dicloxacillin was only 9–17%. However, these calculations may represent an underestimation. First, the uptake of oral flucloxacillin is variable. Dijkmans et al. [22] demonstrated insufficient drug absorption in 13% of patients and proposed an oral absorption test at the time of switching from intravenous to oral treatment. Second, the high protein binding (97% for dicloxacillin, 95% for flucloxacillin) implies a low free fraction to mediate the antibiotic effect. However, estimating the unbound concentration using a fixed protein binding factor may underestimate unbound concentrations, especially in critically ill patients [23,24,25]. Most likely, this phenomenon is caused by hypoalbuminaemia leading to higher free fractions, which is not only present in patients requiring critical care, but also common among patients with severe bacterial infections [24]. Finally, recent animal data [26] suggest a relatively low PK/PD target (20%fT > 0.25xMIC for a 2-log reduction of MSSA), implying that previously calculated PTAs for flucloxacillin in MSSA infections might be too low [26].
Another strategy for better PTA is to prolong the half-life of flucloxacillin through interference with tubular secretion by adding probenecid to the treatment [12]. Up to 5.5-fold improvements of fT > MIC have been demonstrated through alteration of the concentration-time curve shape by combining these drugs. This strategy could provide better conditions to achieve patient compliance through longer dosing intervals with unaltered PTA [27].
Thus, there are several uncertainties in the assumptions used when calculating a low PTA for flucloxacillin in the treatment of MSSA infections, and there are also measures to be taken to optimize treatment conditions. Therapeutic drug monitoring (TDM) was not performed on the patients included in this study; however, one of the two patients who relapsed had a high body weight, and hence might have been underdosed. It is possible that a structured algorithm utilizing an oral absorption test and TDM might aid in the selection of suitable patients and optimizing dosing strategies if oral flucloxacillin follow-up treatment is considered.
Another concern in flucloxacillin use is the potential adverse effects, especially idiosyncratic hepatotoxicity [28]. In this cohort, the frequency of documented side-effects requiring cessation of oral flucloxacillin was 6%, including 1 patient (3%) with hepatotoxicity. All side-effects were reversible after switching drug. It has been estimated that flucloxacillin-associated liver damage will occur in 1 in 7 000 patients in a general population, but the risk varies with age, being 15-fold higher in patients aged over 70 years compared to patients under 50 years [29]. Female sex, HLA-B*57:01 genotype, and pre-existing kidney stones have also been associated with elevated risk for hepatotoxicity during flucloxacillin treatment [30]. In comparison, the incidence of hepatotoxicity has been reported to be 3% for fluoroquinolone treatment [31] and 1% for rifampicin monotherapy [32]. In a prospective study on treatment of diabetic foot osteomyelitis, 40% of patients experienced adverse events, most commonly gastrointestinal which were all attributable to rifampicin. Induction of metabolic enzymes (e.g., CYP3A4) leading to extensive drug-drug interactions further complicates rifampicin usage [32]. Another serious adverse event after antibiotic treatment is Clostridioides difficile infection. Interestingly, the adjusted odds ratio (aOR) for dicloxacillin is similar to that of ciprofloxacin, despite being a more narrow-spectrum antibiotic. In that regard, levofloxacin seems to be a better option among fluoroquinolones, while clindamycin, recommended as second-line therapy by IDSA and SPILF, was associated with the highest aOR of all studied antibiotics in a matched case-control study [1, 4, 33]. Thus, all potential treatment options for vertebral osteomyelitis have their pros and cons, and it is crucial to be aware of these risk factors when selecting the therapy least likely to cause harm to the individual patient.
Limitations of this study include its retrospective nature, including the possibility that cases were not found due to coding errors, the small number of patients, and the low occurrence of relapses. From this cohort, it is not possible to draw conclusions regarding the optimal treatment duration. Moreover, a larger cohort would provide a better estimate of the safety and efficacy of flucloxacillin treatment in vertebral osteomyelitis.
In conclusion, prolonged flucloxacillin administration as an oral follow-up for MSSA vertebral osteomyelitis resulted in an 83% (20 of 24) clinical cure rate in this small retrospective cohort. The optimal treatment duration is unknown, but 12 (–16) weeks may be sufficient even in the presence of abscesses, provided that adequate drug absorption is ensured. A prospective study on treatment duration utilising TDM to optimize conditions for target attainment might shed further light on the optimal usage of flucloxacillin in the setting of MSSA bacteraemia complicated by vertebral osteomyelitis.


Comments (0)