
Remember me
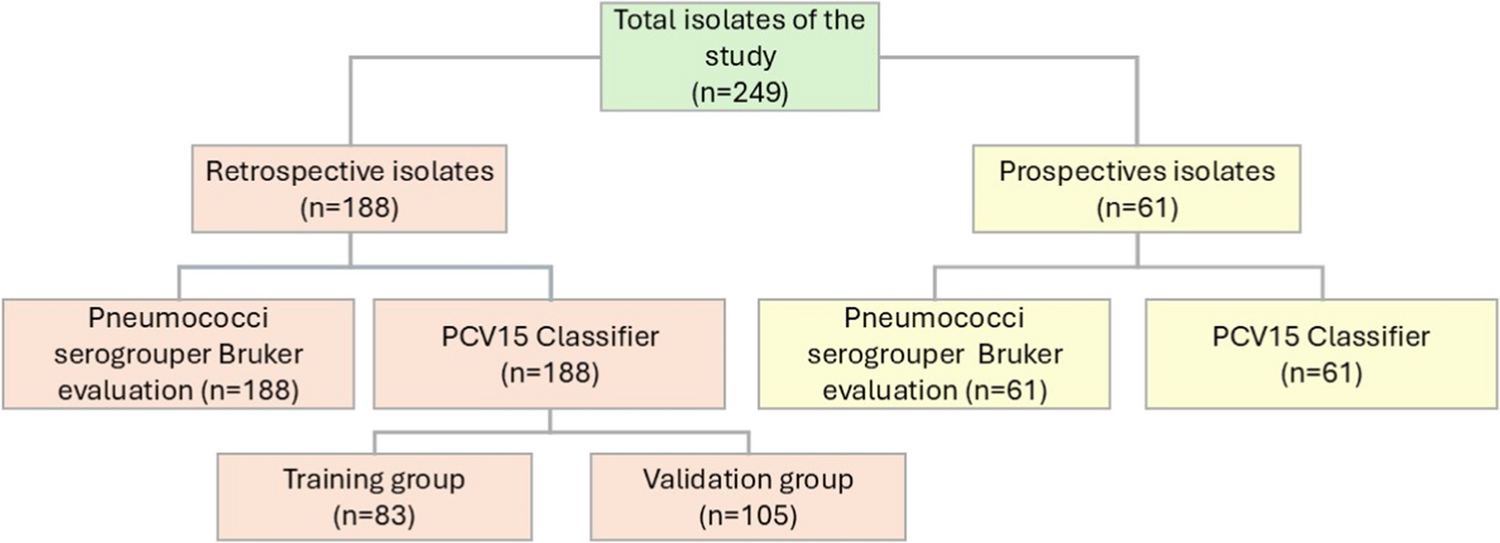

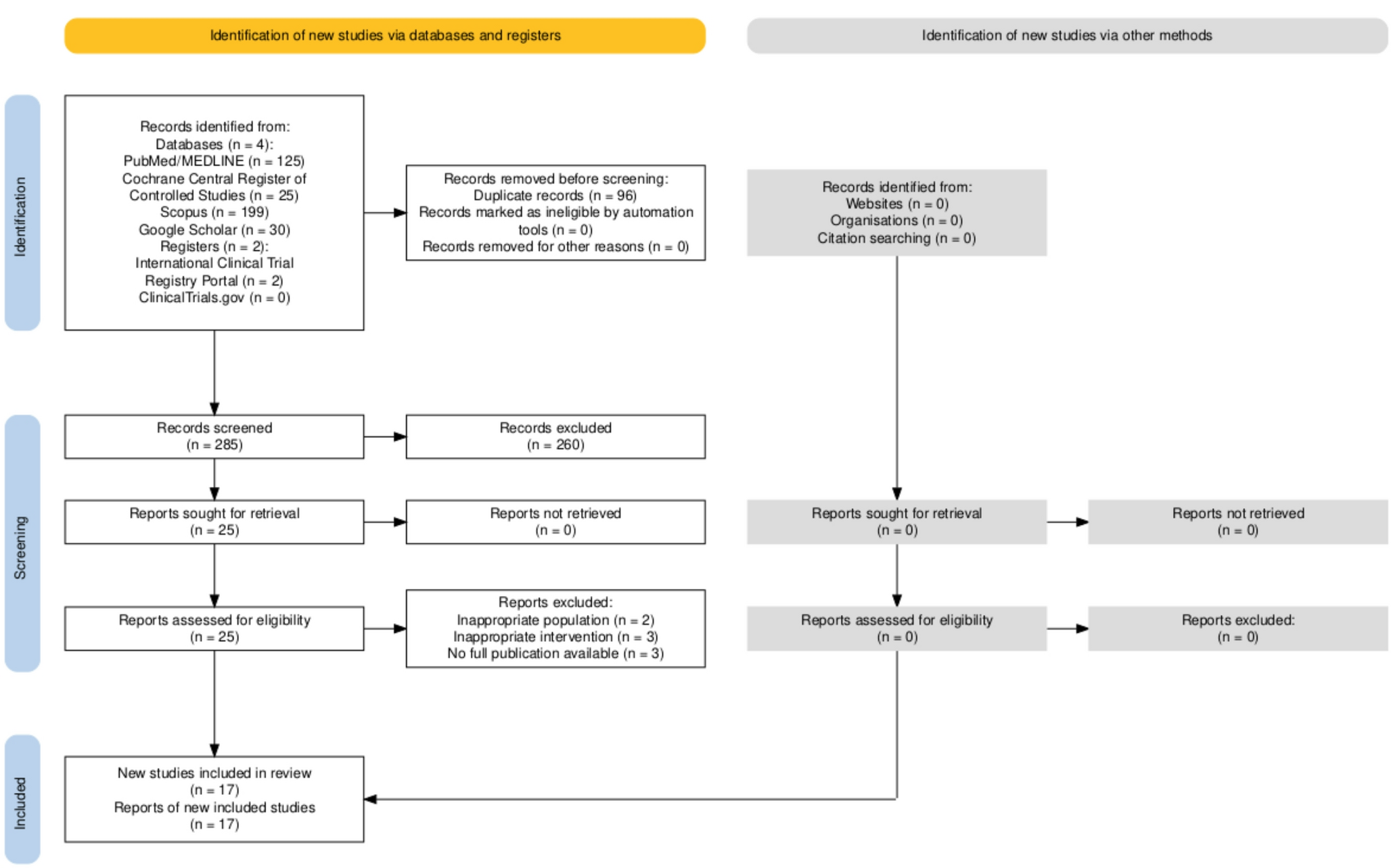
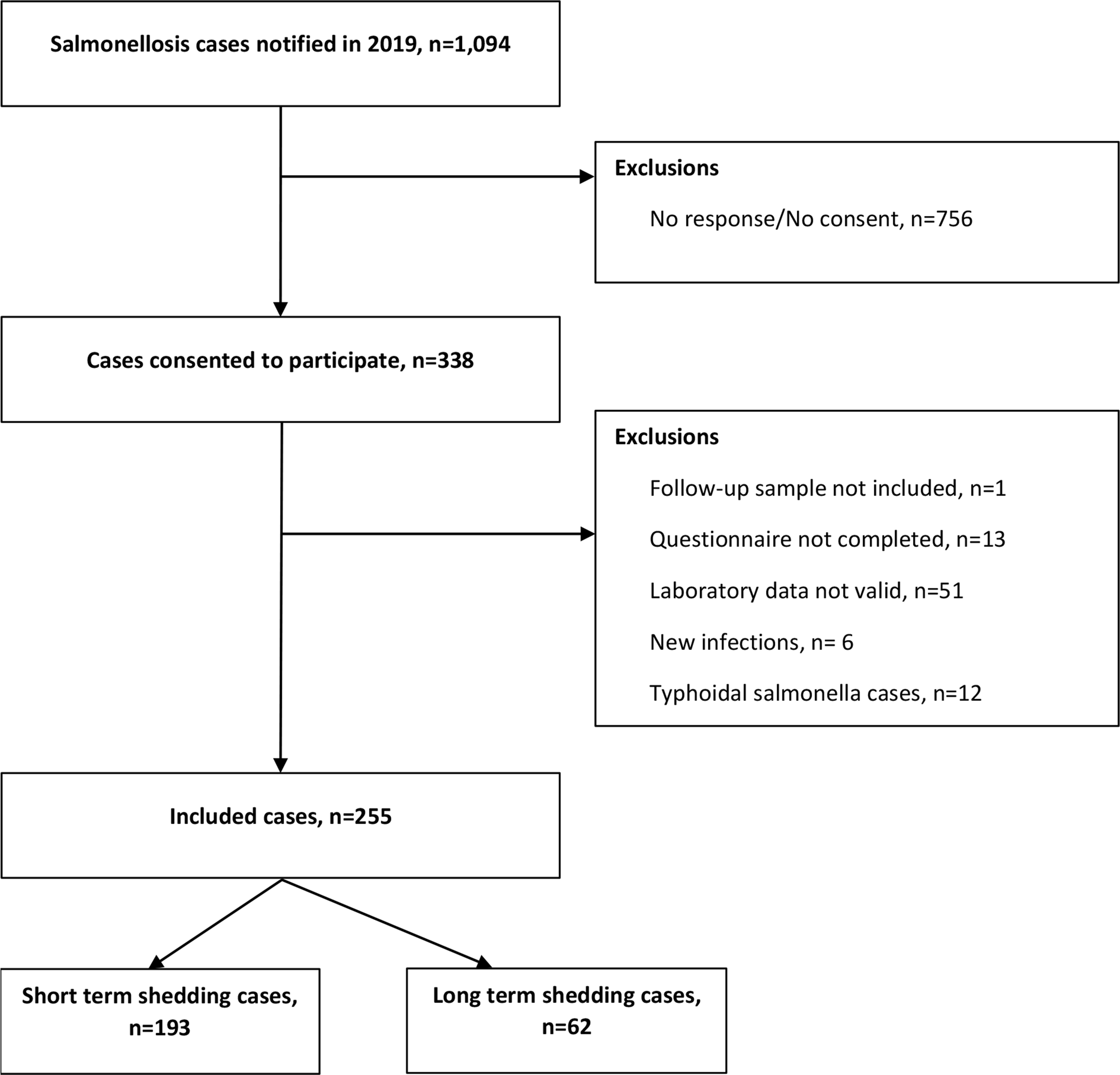
During the study period, a total of 1,094 cases of salmonellosis were notified to MSIS, and all were invited to participate in the study. Of these, 338 (31%) gave their consent to participate, of which 25% (n = 83) were excluded because: (i) they did not send a follow-up stool sample, (ii) did not complete the questionnaire, (iii) the laboratory data was not valid, (iv) the follow-up sample indicated a new infection, or (v) the laboratory result was a typhoidal Salmonella. Further details are presented in the inclusion summary flowchart in Fig. 1.
Fig. 1
Inclusion summary flowchart, MoMIR study, Norway, 2019
After applying the exclusion criteria, 255 individuals were included in the study, resulting in 23% participation rate. After analysis of the genomes of the initial isolates and the follow-up samples, 62 participants (24%) were classified as LTS, and 193 (76%) as STS. Age was reported by 250 (98%) of the participants, ranging from 1 to 91 years old; median age 51 years (IQR: 25). Participants from all counties of Norway replied to the survey, with 13% of them having residency in Trøndelag, 13% in Oslo, and 11% Vestland. When comparing the proportions of the participant demographic characteristics with those of all Salmonella cases notified in 2019, study participants were representative by age, sex and county of residence with a slightly overrepresentation of older adults, 40–69 years old (see Online Resource 2, Table S1).
Serotypes identifiedS. Enteritidis was the most common serotype identified in 42% (n = 107) of the isolates, followed by S. Typhimurium in 11% (n = 27) and S. Agbeni or Bron in 9% (n = 22). During the study period, an outbreak of Salmonella Agbeni or Bron (22 cases) linked to imported dried fruits occurred in Norway. Among these serotypes, S. Enteritidis and S. Typhimurium showed a 21% (23/107) and 19% (5/27) LTS frequency, respectively. The highest percentage of LTS was 45% (10/22) among participants identified with S. Agbeni or Bron, followed by 29% (2/7) among S. Coeln and 25% (4/16) among monophasic S. Typhimurium cases. The lowest percentage of LTS was 11% (1/9) among S. Newport cases.
Assessing risk factors for long-term shedding infectionSome of the main risk factors that were assessed for the risk of LTS before reaching the final multivariable model are included in Tables 1 and 2 (further details on subcategories and additional factors provided in Online Resource 2, Table S2 and S3. Due to the length of the questionnaire and the large number of factors assessed, only a subset of the main risk factors is presented in the main article. A complete list of all questions included, and factors assessed can be found in the study questionnaire (Online Resource 1).
Table 1 Partial results from univariable analysis assessing risk factors for long-term shedding infections of non-typhoidal Salmonella. Here some of the risk factors that were assessed before reaching the final multivariable model are presentedTable 2 Results from multivariable analysis, assessing risk factors for long-term shedding infections of non-typhoidal SalmonellaAmong the 255 participants, around 32% (n = 82) reported animal contact up to a week before having the infection detected and 53% (n = 135) after recovering from the disease. More than half (61%, n = 156) of the participants reported travel abroad the last week before having the infection detected (Table 1).
About half (54%, n = 138) of the participants received regular medication (not related to Salmonella), including 13% (n = 33) using antacids, 9% (n = 24) food supplements, 2% (n = 4) using corticosteroids, and 45% (n = 116) “other regular medication” (Online Resource 2, Table S3). 18% (n = 45) had a history of abdominal surgery prior to the infection, and 84% (n = 215) reported having received medication in the acute phase of the Salmonella infection. Medication received during the acute infection included among others, diarrheal medication (n = 89, 35%), use pre-or probiotics (n = 79, 31%) and antibiotics (n = 65, 25%) (Table 1).
Moreover, 3% (n = 8) of participants reported having a lactose free diet (not related to infection), and none of them reported being vegetarian, vegan or pescetarian (Online Resource 2, Table S2). Also, 33% participants (n = 76) used pre- or probiotics in their diet. When clarifying what type of pre or probiotics they used, 27% (n = 68) indicated sour milk or yogurt with probiotics, 5% (14) drops, tablets or powder with pre-or probiotics, and 3% (n = 7) used “other pre- or probiotic products”.
In our multivariable analysis (Table 2), we observed that participants in age group 0–5 years were 6.7 times more likely to shed Salmonella five weeks after infection (LTS) compared to participants in age group 18–44 years (aOR = 6.71, 95%CI: 1.67–26.94). Participants using regular medication, not related to the acute gastrointestinal infection, were two times more likely to be LTS (aOR = 2.17, 95%CI: 1.02–4.64) compared to those who did not. However, when we explored the detailed questions about regular medication in the univariable analysis, “corticosteroids” and “other medication” was associated with increased odds, but in our multivariable analyses (excluding the overall “regular medication” variable in this analysis), none of the single available options in the questionnaire (antacids, corticosteroids, immunosuppressives, insulin, food supplements etc.) were associated with increased risk of LTS. Also, participants who reported having a lactose free diet or used “other pre- or probiotic products” in their diet (even though the numbers are small) were more likely to be categorised as LTS compared to those who did not, with aOR 7.24 (95%CI: 1.48–35.40) and 8.68 (95%CI: 1.39–54.30) respectively. Regarding serotypes, the participants identified with S. Agbeni or Bron were 6 times more likely to be categorised as LTS compared to the participants with S. Typhimurium (aOR = 6.29, 95%CI:1.40–28.16).
We should note that the use of “other pre- or probiotic products” in their diet, reported by 3% of participants, was not associated with higher odds of LTS in the univariable analysis (OR:4.37, 95%CI: 0.95 – 20.08) but became significant when included in the multivariable analysis (aOR: 8.68, 95%CI: 1.39–54.30). Among the rest of the assessed risk factors, receiving food supplements as part of the medical treatment for the NTS infection, reported by 11% of participants, was associated with higher risk of LTS in the univariable (OR:2.39, 95%CI: 1.04–5.46), but this association was not significant in the multivariable analysis.
SymptomsSymptoms during infectionOnly four participants (1.6%) were asymptomatic (3 STS and 1 LTS). The most frequent symptoms reported by the participants during their infection were diarrhea (90%), abdominal pain (67%) and fever (64%). Other common symptoms were nausea (39%), mucus in stool (36%), blood in stool (24%) and vomiting (23%) (Table 3). No difference was observed in the distribution of symptoms among participants with STS and LTS (chi square p-values > 0.05).
Table 3 Symptoms during infection as reported by study participants and evaluated based on shedding phenotype of non-typhoidal SalmonellaProlonged symptomsAt the time of the second stool sample collection, approximately five weeks after the initial sample, 35 participants (14%) reported experiencing symptoms. The most common prolonged symptoms were abdominal pain (n = 15, 6%), mucus in stool (n = 12, 5%), and diarrhea (n = 9, 4%) (see Online Resource 2, Table S4 for further details). Duration for the reported symptoms could not be determined based on our questionnaire. No difference was observed in the distribution of prolonged symptoms between participants with STS and LTS (chi square p-values > 0.05).
Hospitalisation31% of the participants (n = 80) were hospitalised, 30% among those with STS and 37% among those with LTS (no difference observed, chi square p-value = 0.264). Among 79 of the hospitalised participants with available information, reported duration of hospital stay ranged from 1 to 18 days, median = 4 days (IQR:3). No difference was observed in the median duration of hospitalisation among LTS and STS (rank-sum test p-value = 0.122). Moreover, no difference was observed in the distribution of hospitalisations among participants infected with different Salmonella serotypes (chi square p-value = 0.824). Further details regarding hospitalisations by serotype and by short-term shedder and long-term shedder phenotypes are presented in Online Resource 2, Table S5.
Antimicrobial resistanceThe in-silico analysis of AMR determinants from the Salmonella isolates recovered from the participants, identified Quinolone resistance as the most frequent AMR genotype with 16% (n = 41), followed by tetracycline (n = 35, 14%) and resistance to β-lactams (n = 33, 13%). Only one isolate was identified with a Lincosamide resistance genotype. A multi-drug resistance genotype (resistance to more than three antibiotic classes) was identified in 30 isolates (12%), however only a single isolate was predicted to have an ASSuT phenotype. Of all the investigated antimicrobial families and genotypes, only Fosfomycin resistance was significantly associated with LTS phenotype (chi-square p-value = 0.017, n=4) (Table 4).
Table 4 Distribution of detected antibiotic resistant genotypes in participants by short-term shedder and long-term shedder phenotypes of non-typhoidal Salmonella
Comments (0)