Study design and aims
This pilot prospective study compared outcomes for 23 participants receiving the FN intervention to 23 historical control participants who did not receive the intervention. The primary aim was to understand how a FN impacts interdisciplinary outpatient appointment attendance following admission. Seven additional participants that were approached about the study but did not enroll were included to evaluate differences from those who consented and enrolled in the study. The pilot study also explored two secondary analyses: (1) impact of the FN intervention on mental health and readmission rate outcomes and (2) parent satisfaction and interaction with the FN throughout the study.
FN training
A FN was hired based on her experience working as a medical assistant including proficiency calling and interacting with families to specifically engage treatment adherence. She received 10 h of one-on-one training from a clinical psychologist and registered dietitian specializing in eating disorders on the following intervention elements: research ethics and participant protections, self-management knowledge as it relates to restrictive eating disorders, and interpersonal strategies for individual- and family-based facilitation of change. For instance, topics of training included: navigating personal disclosure, fostering connections between a parent and adolescent, understanding and utilizing reflective listening skills, and how to manage parent/guardian distress during the intervention period. The FN was also given a 30-page manual developed by the lead author, a clinical psychologist and the second author, a registered dietitian; informed by feedback from an interdisciplinary team. Over the course of the intervention, the FN met weekly with members of the larger interdisciplinary medical team including a clinical psychologist, registered dietitians, and medical doctor, to address any patient or parent concerns and provide an opportunity for the FN to debrief about any questions she had over the course of the week.
Parent and adolescent participants
The FN intervention was conducted with parent participants of adolescent patients admitted for medical stabilization to the Adolescent Medicine eating disorder unit in a large children’s hospital from August to December 2023. To be included in the study, an individual had to be the parent of a current patient aged 10–17 on the medical inpatient eating disorder unit with a primary diagnosis of AN (restricting, binge/purge) or AAN) who had a discharge plan to outpatient care. Additionally, to be eligible for the intervention, the parent had to enroll their child in the outpatient program, which included up to 24 sessions of individual and family based therapy, at least one medical or nursing visit within three months of discharge, at least one nutrition visit within three months of discharge, and an 8-week virtual group therapy program for the patient only (RAPP: Recovery and Prevention Program), which met virtually for one hour every Tuesday, Wednesday and Thursday for a total of 24 h of group therapy). Exclusion criteria included: (1) cognitive limitation that prevented parents from completing electronic/web-based surveys; (2) inability to speak and read in English or Spanish; or (3) parents of patients who were recommended for a higher level of care after discharge or who had previously been admitted to a medical eating disorder inpatient unit. If all criteria were met, a member of the study team contacted one or both parent(s)/legal guardians via phone to confirm eligibility and describe the purpose of the study. If a parent was interested in participating in the study, a separate call was made to consent the parent and obtain assent from the adolescent for the study using an Institutional Review Board approved online consent form process through REDCap software.
Historical controls were matched 1:1 to cases from a pool of prior patients admitted to the eating disorder unit without access to a FN at discharge but offered and agreeing to attend the full outpatient program including medical, nutrition, and mental health follow-up appointments. The historical control patients were discharged from the hospital from September 2021-August 2023. We aimed to match controls with the FN patient cases based on age (± 2 years), gender, diagnosis, and primary language (English or Spanish). Due to sample size limitations, as many historical patient records were missing self-reported mental health outcomes, some patients were only able to be matched on gender identity, age, and primary language. Patients who did not have identical diagnoses were matched as closely as possible; for instance, a male 15-year-old patient with anorexia nervosa- restricting type would be matched to a male 15-year-old patient with atypical anorexia nervosa if there was not another 15-year-old male with AN-R. Control data was obtained through medical record review. Control data was obtained through medical record review. All patients and parents (historical control and FN intervention groups) received the same medical and behavioral health interventions while admitted.
FN intervention
For the intervention, the FN met with the family either in person on the inpatient unit before discharge or via a scheduled 60-minute introduction call. During this meeting, the FN followed a detailed script that described the purpose of the intervention, the FN role and the upcoming transition to outpatient care including the components of that care (e.g., medical doctor, registered dietitian, registered nurse, and individual, family, and group therapy visits). For instance, the FN spent time explaining to families that their child would receive three types of mental health treatment while outpatient: weekly to biweekly individual therapy, weekly to biweekly family-based therapy, and 8 weeks of a virtual group therapy program that met 3 h each week. The FN described the differences between these therapies, the purpose of each, and the value of each in their child’s recovery. The FN reviewed information with families about expectations regarding meals and physical activity when returning home, including meal schedules and how to manage food refusal. The FN answered parent questions and attempted to solve immediate concerns when appropriate. After this initial visit, the FN called, emailed (via secure online portal), or texted families weekly for three months post-discharge to assist with attendance barriers and answer family questions or concerns. These weekly contacts included the opportunity for the FN to check in with parents to address any concerns regarding their child’s appointments, adherence to medical and psychological recommendations and overall recovery. The FN documented all contact with families including how often families reached out and for what reasons as well as the time spent each day interacting with families.
Measures
Demographic characteristics (age, gender, race/ethnicity) were self-reported by the adolescent in both the historical control and FN intervention groups via online surveys completed during weekly group therapy. Patient insurance status, primary language spoken at home, AN diagnosis type, and mood and anxiety disorder comorbidities were collected through medical chart review.
Change in patient weight was assessed by calculating %mBMI (BMI/medianBMI for age and sex based on 2020 CDC growth chart) at time of hospital discharge and 3 months post discharge.
Mental health diagnoses were obtained from the patient’s psychological diagnostic intake during their inpatient admission by a clinical psychologist. Readmission (yes/no) within six months of discharge was also determined based on medical chart review. Patients readmitted to any inpatient eating disorder program within 6 months of discharge were classified as readmitted. To assess impact on treatment adherence we measured both total number (frequency) and percent of total appointments (rate) attended based on FN documentation. Specifically, for rate we counted the number of appointments attended versus cancelled or not attended out of the number of outpatient appointments scheduled in the first three months after discharge. Frequency at individual appointment types was calculated by summing the total number of visits attended. Rate was calculated as the percent of scheduled appointments attended for each appointment type. We used multiple methods because the total number of scheduled appointments for each visit type varied by patient. Attendance at RAPP was assessed as a percentage of the available RAPP groups (N = 21–24) that the patient attended. While attendance outcomes included both total number (frequency) and percent of total appointments (rate), it is important to highlight what types of medical and therapeutic visits were offered as part of the outpatient eating disorder treatment program. Families were not able to remain in the outpatient program unless they agreed to be a part of every visit type: individual therapy, family-based therapy, medical/nursing visits, nutrition and RAPP/group therapy:
Family based therapy visits
Patients were scheduled for up to 12 family therapy sessions led by a licensed clinical psychologist over the first 6 months starting 5 days following discharge from the hospital. Most appointments were scheduled for 1 h every 2 weeks. At minimum, one parent or caregiver was expected to be present for the duration of the visit, but often multiple caregivers or siblings were invited. The purpose of these visits was to empower parents to assume responsibility for preparing, measuring, and plating all meals and snacks for their child. At these visits, we often advised parents on how to manage food refusal, improve communication around food and body image, and continue to encourage regular patterns of eating without purging or physical activity until weight is restored.
Individual therapy visits
Patients were scheduled for up to 12 individual therapy sessions led by a licensed clinical psychologist over the first 6 months starting within 5 days following discharge from the hospital. Most appointments were scheduled for 1 h every 2 weeks. These sessions primarily used a Cognitive Behavioral Therapy approach aimed at assisting patients with completing meals, facing fear foods, and managing body image disturbance. Specific coping strategies often utilized included behavioral activation, cognitive restructuring, and exposure and response prevention in the context of food exposures.
Medical doctor or registered nurse visits
Patients were scheduled for a minimum of one outpatient appointment with a MD or RN typically 2–4 weeks after discharge to assess for medical stability and weight gain progress. If physical health concerns (e.g., weight loss since discharge, decreased heart rate, etc.) were identified during that visit, but the patient did not warrant admission, the patient would be scheduled for a follow up MD or RN visit within 1 month. If medically stable, the patient would typically be scheduled for a follow up within 3 months.
Registered dietitian (RD) visits
Patients were scheduled for a RD visit within the first 1–2 months following discharge. Similar to MD/RN visits, if there were concerns about nutritional intake or if the RD felt the family would benefit from more regular support follow up would be scheduled within 1 month. If no concerns were noted at the first outpatient appointment, a patient was typically scheduled for a follow up 2 months later. The purpose of these visits was to educate parents and patients on following the outpatient meal plan although parents were expected to prepare, measure, and plate all meals and snacks for the patient.
RAPP (Recovery and Prevention Program) visits
RAPP is an 8-week virtual group therapy program for the patient only. Groups met virtually for one hour every Tuesday, Wednesday and Thursday for 1 h (a total of 24 h of group therapy). Groups included nutrition content led by a registered dietitian, Cognitive Behavioral Therapy content led by a clinical psychologist, and Acceptance and Commitment Therapy content led by a clinical psychologist. Approximately 8–15 patients attended group each week. Enrollment is rolling such that patients would enroll in RAPP immediately upon discharge allowing them to attend the first Tuesday they were home, at most 7 days after discharge.
Mental health outcomes
To assess changes in mental health symptoms over the course of the intervention, adolescent patients completed weekly standardized measures of depression, anxiety, and eating disorder symptoms during RAPP appointments. The week 1 survey served as their baseline data and the week 8 survey as their post-intervention data point. Specifically, patients completed:
(1)
The 9-item Patient Health Questionnaire (PHQ-9) [39] was used to assess depression symptoms. The PHQ-9 has demonstrated strong sensitivity, specificity and construct validity among large representative samples of adolescents [40]. Increasing PHQ-9 scores are significantly correlated with increasing levels of functional impairment, as well as parental report of internalizing symptoms and psychosocial problems [41].
(2)
The 7-item Generalized Anxiety Disorder (GAD-7) [42] was used to measure anxiety symptoms. The psychometric properties of GAD-7 scores have been tested and well validated [43, 44].
(3)
The 21-item Eating Disorder Questionnaire (EDEQ) [45] was used to measure disordered eating symptoms. The EDEQ consists of four subscales measuring: (1) Restraint, (2) Eating concern, (3) Shape concern, and (4) Weight concern. The EDEQ has a total score that is an average of the four subscales and is used as a cut-off point for eating-disorder pathology. The EDEQ has demonstrated strong internal consistency and reliability, concurrent validity, and discriminant validity [46].
Parent satisfaction with the pilot intervention was assessed through quantitative parent satisfaction ratings taken each month during the 3-month intervention period. Each parent was given the opportunity to complete three satisfaction surveys (Appendix) over the course of the intervention. The satisfaction measure was developed from an intervention for binge eating disorders to assess feasibility and acceptability measures [47] and was specifically used in this study to assess the parent’s satisfaction with the intervention and to provide the parent with the opportunity to provide feedback regarding what they liked and what they might add to or change about the intervention. The satisfaction measure asked parents to rate how helpful the FN was with multiple aspects of care and to indicate what was most helpful about the intervention in their child’s recovery (Appendix). Parent responses to the question “What has been most helpful/valuable about having a family navigator?” were reviewed by the authors to determine broader suggestions for improvement in the intervention for future studies. Individual responses were then reviewed to verify inclusion in categories until consensus was reached as to which category of improvement each response best fit.
Finally, FN engagement was measured by counting the number of calls or texts from the FN to the families. The content of each text message and call was reviewed by the study authors to identify the general purpose of the communication (e.g., appointment related question, nutrition related question, etc.). We report the frequency of each of general type of communication in the results section.
All patient and parent measures were completed using REDCap, a secure, web-based, HIPAA-compliant database used to collect medical research data. Parents were compensated $10 for each monthly satisfaction survey they completed.
Statistical analysis
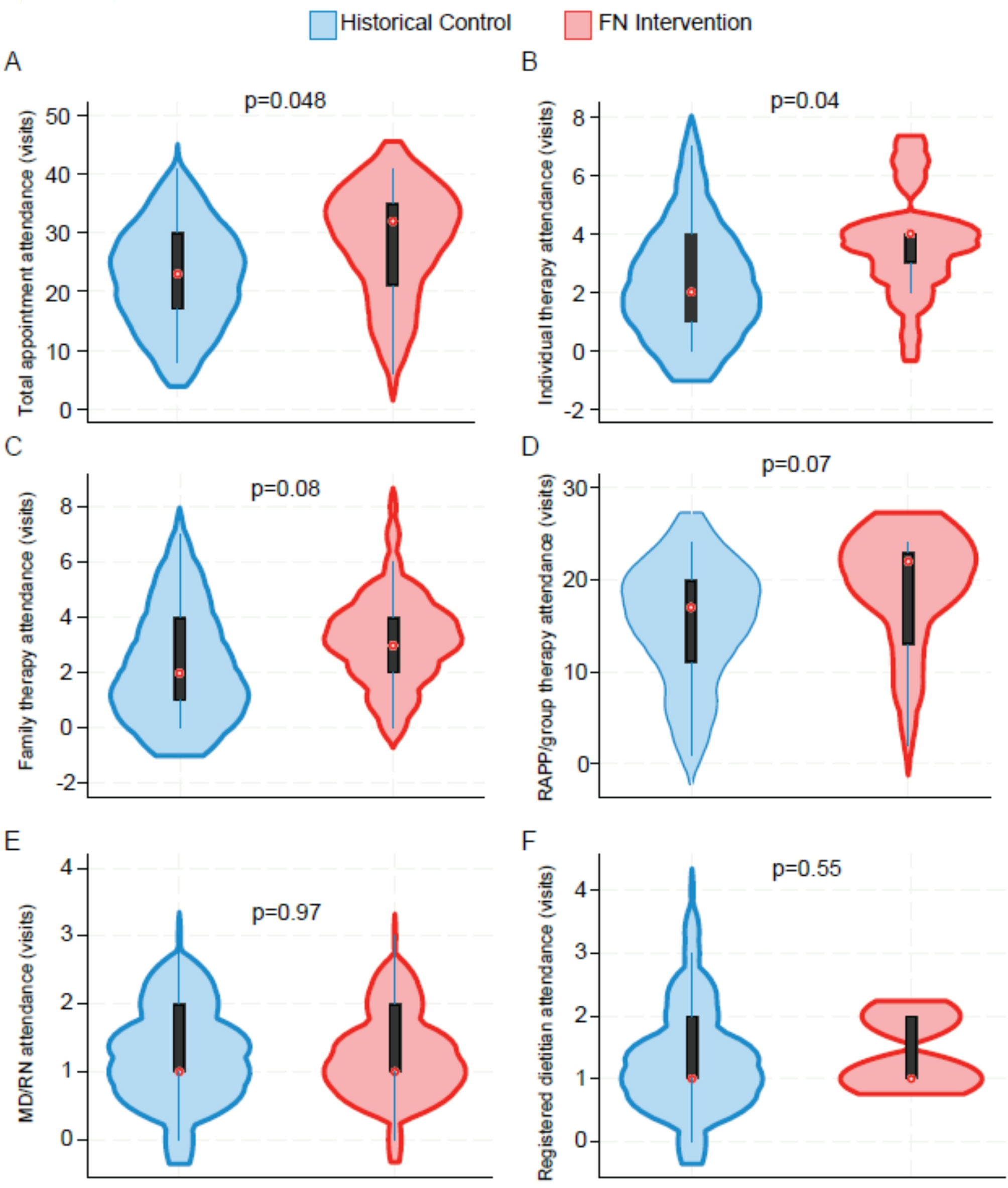
Patient characteristics and outcome data are reported as frequencies and proportions for categorical variables and as median and interquartile range (IQR) for continuous variables. Differences between groups were determined using the Fisher’s exact tests for categorical variables and Wilcoxon rank-sum test for continuous variables. Violin plots were used to present the attendance frequency between FN intervention and historical control groups. A logistic regression was used to analyze the relationship between degree of visit attendance and mental health and weight related outcomes. We created yes/no variables for whether the patients had a decrease in mental health symptom scores (GAD-7, PHQ-9, and EDEQ) from week 1 (baseline) to week 8 and whether %mBMI < 100%. Then, we ran logistic regressions for all 46 patients adjusting for FN intervention group (Yes/No). A mixed-effects linear regression analysis was used to assess changes in %mBMI. Analyses were performed on Stata MP version 18.5 [48]. A p-value of < 0.05 was considered statistically significant.


Comments (0)