
Remember me
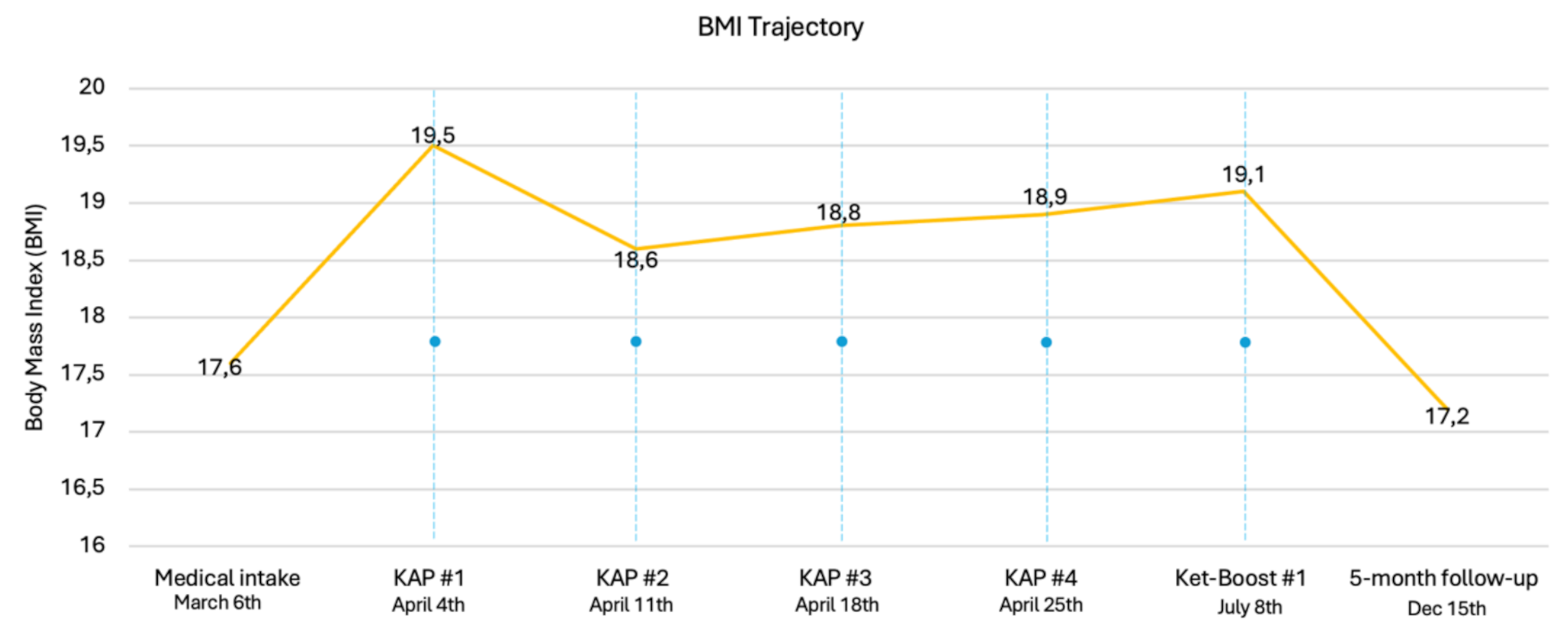

Descriptive data from clinical assessments—including indications for KAP, medical and psychiatric history, current and prior psychological and pharmacological treatments, diagnoses, reported ketamine side effects, and synopses of KAP sessions—were documented by the treatment team, consisting of the medical doctor MD, clinical psychologist, and psychiatric nurse. Additionally, medical data from the patient’s records, such as age, Body Mass Index (BMI), and ketamine injection doses are reported. Weight was recorded at the clinic during the medical intake, at each KAP session, and at the first ketamine booster session. At 5-month follow up, weight was self-reported as the patient had moved abroad. BMI (see Fig. 1) was calculated using the patient’s height as measured at the initial assessment, combined with her weight at each respective time point.
Fig. 1
BMI trajectory from medical intake to 5-months follow-up. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. BMI: Underweight: <18.5, Normal weight: 18.5–24.9: Overweight: 25–29.9. The blue dots and lines represent KAP and ketamine booster sessions
Self-report assessmentsSelf-reports were completed at five key time points: approximately one month before the first KAP session, three weeks after the final KAP session, one day prior to the first ketamine booster dose, as well as six weeks and five months following the final ketamine booster dose. Apart from the Eating Disorder Examination Questionnaire (EDE-Q), self-reports were completed digitally.
Table 1 visually outlines the timeline for medical intake assessment, self-report assessments, KAP sessions and ketamine booster doses. The entire time frame from the medical intake to the 5-month follow-up spanned just over nine months Assessment measures used are detailed below.
Table 1 Timeline for the medical intake assessment, self-report assessments, ketamine-assisted psychotherapy, and ketamine booster sessionsThe Eating Disorder Examination Questionnaire (EDE-Q v. 16.0) [37] measures the attitudinal features and core behaviors of EDs, such as food restriction, binge eating and inappropriate compensatory behaviors, over the past 28 days. It includes four clinically derived subscales: Dietary Restraint, Eating Concern, Weight Concern, and Shape Concern, each consisting of five to eight items. These subscales are used to calculate a global EDE-Q score. The 22 attitudinal items that comprise the global score are rated on a seven-point scale (0–6), with higher scores indicating greater ED pathology. The literature indicates that a global score at or above 2.8 may indicate clinically significant ED pathology [38]. The Norwegian translation of the EDE-Q has shown good psychometric properties in a non-clinical sample of female university students [39]. A validated Norwegian EDE-Q version was used as part of the routine clinical assessment in this study.
The Patient Health Questionnaire (PHQ-9) [40] is the self-report depression module of the PRIME-MD diagnostic instrument for mental disorders. It is designed for use in primary care and taps into each of the nine DSM-IV/ICD-10 depression criteria on a 4-point Likert scale: «Not at all (0), «Some days [1], «More than half the days» [2] and «Nearly every day» [3]. Item scores are summarized, generating a global score. The following cut-off scores are recommended for the PHQ-9 5–9: Mild symptoms of depression, 10–14: Moderate symptoms of depression, 15–19: Moderately severe symptoms of depression and 20–27: Severe symptoms of depression [41]. A validated Norwegian PHQ-9 version [42] was used as part of the routine clinical assessment in this study, which assesses symptoms of depression over the previous two weeks.
The Generalized Anxiety Disorder Questionnaire (GAD-7) [43] is a self-administered screening tool and severity measure for general anxiety disorder (GAD). Seven questions are scored on a 4-point Likert scale based on the severity of the respondents’ symptoms the previous two weeks. Response options include «not at all» (0), «several days» [1], «more than half the days» [2] and «nearly every day» [3]. A total score is calculated by adding together the seven item scores, with a minimum score of 0, and a maximum score of 21. Higher scores reflect higher levels of anxiety and associated functional impairment and disability. Cut-off scores of 5, 10, and 15 are interpreted as representing mild, moderate, and severe levels of anxiety. When GAD-7 is used for screening purposes, follow-up evaluations are recommended at total scores at or above 10. A validated Norwegian GAD-7 version [42] was used as part of the routine clinical assessment in this study.
The Montgomery–Åsberg Depression Rating Scale (MADRS) [44] is a 10-item clinician rated assessment of depression symptoms and severity, and suicidal thoughts. As part of the routine clinical assessment at the Axon Clinics, patients self-report MADRS item number ten (MADRS-10) which captures suicidal ideation the previous week, e.g., the feeling that life is not worth living, that a natural death would be welcome, and preparations for suicide. The response options for item 10 are as follows: “Enjoys life or takes it as it comes” (0), “Weary of life. Only fleeting suicidal thoughts” [2], “Probably better off dead. Suicidal thoughts are common, and suicide as considered as a possible solution, but without specific plans or intention” [4] and “Explicit plans for suicide when there is an opportunity. Active preparations for suicide” [6]. The MADRS item 10 has been reported to be well-suited for ongoing assessment of suicide risk when using rapid antidepressants like ketamine [45].
The EuroQol Five Dimension-Five Level (EQ-5D-5 L) [46] is a self-report instrument designed to assess current (i.e. at the time of assessment) generic health related quality of life (QoL) on five descriptive dimensions: Mobility, Self-Care, Usual Activities, Pain/Discomfort, and Anxiety/Depression. Each dimension has five descriptive response options: [1] «not /no problems» [2], «slight problems» [3], «moderate problems» [4], «severe problems», and [5] «unable to» (Mobility, Self-care, Usual Activities), «extreme» (Pain/Discomfort), or «extremely» (Anxiety/Depression). A common way of scoring the EQ-5D-5 L is to combine the digits of the five dimensions into a 5-digit “profile” (e.g., 1-1-2-3-1) describing the patient’s overall health state. In addition, respondents rate their current health state using a 0–100 scale with endpoints labelled “Worst imaginable health state” (0) and “Best imaginable health state” (100). A validated Norwegian EQ-5D-5 L version [47] was used as part of the routine clinical assessment in this study.
The Acceptance and Action Questionnaire v.2 (AAQ-II) [48] is a one-factor, 7-item self-report measure of psychological inflexibility. The questionnaire can be administered weekly or bi-weekly to track the respondent’s psychological flexibility (or inflexibility) skills in their daily life, and includes statements such as «I worry about not being able to control my worries or feelings», «It seems like most people are handling their lives better than I am», «Emotions cause problems in my life» etc. Items are scored on a Likert-scale ranging from 1 (Never true) to 7 (Always true) and are summarized to calculate a total score. Higher scores indicated greater levels of psychological inflexibility, and greater emotional distress. A score of 25 or higher reflects significantly reduced psychological flexibility, often associated with symptomatic presentations. A validated Norwegian AAQ-II version [49] was used as part of the routine clinical assessment in this study.
The Ketamine Side Effect Screening Tool (KSET) [50] is a clinical tool designed to assess side effects associated with ketamine treatment and support clinicians in their decision-making processes before, during, and after treatment. In this case report, a modified, non-validated Norwegian version of the KSET was used. The patient rated their experiences with 20 potential side effects over the past month on a 4-point Likert scale: “Never” (0), “Mild” [1], “Moderate– caused discomfort and/or interference with usual activities” [2], and “Severe– caused significant discomfort and considerable interference with usual activities” [3]. The side effects assessed included: “dissociation,” “hallucinations,” “problems with memory and/or concentration,” “anxiety,” “restlessness/worry/agitation,” “elevated/irritable mood,” “tearfulness,” “drowsiness, fatigue, bodily weakness,” “dizziness, light-headedness, feeling faint,” “headache,” “numbness and/or tingling of body parts,” “abnormal movements,” “vision changes,” “hearing changes,” “dry mouth,” “increased salivation or metallic/unusual taste,” “cardiovascular issues,” “nausea and/or vomiting,” “skin changes,” “feeling unusually hot, sweaty, or cold,” and “problems passing urine.” An aggregated score was calculated (range 0–60), with higher scores indicating greater severity of ketamine side effects.
OutcomesSelf-report assessments and BMISelf-report assessment outcomes are summarized in Table 2. The difference in symptom scores (∆sympt) from the initial to the final assessment are presented in the rightmost column. The plus and minus signs denote whether the scores have increased or decreased. Figures 2, 3, 4, 5, 6, 7 and 8 provide visual representations of ED pathology (EDE-Q), depression (PHQ-9), anxiety (GAD-7), psychological flexibility (AAQ-II), quality of life health state (EQ-5D-5 L), and ketamine side effects (KSET), across all time points. Figure 1 shows the patient’s BMI trajectory from medical intake to 5-months follow-up. At the initial assessment, the patient’s EQ-5D-5 L “profile” was 3-2-4-2-3, indicating moderate problems [3] with mobility, slight problems [2] with self-care, severe problems [4] with usual activities, slight problems [2] with pain/discomfort, and moderate problems [3] with anxiety/depression. From the second to the fifth assessment, the patient’s health profile improved to 1-1-1-1-1, reflecting no reported problems across any of the health dimensions. At the initial assessment, the patient’s KSET scores indicated moderate baseline levels of dissociation, memory and/or concentration problems, anxiety, drowsiness, and tearfulness, as well as mild levels of restlessness, dizziness, nausea, and skin changes. By 5-month follow-up, only mild issues with memory and/or concentration, dizziness, and moderate drowsiness were reported. No new ketamine-related side effects were reported during the treatment period.
Table 2 Self-reports across the 9-month assessment period (March 7th to December 15th, 2024)Fig. 2
Eating disorder examination questionnaire (EDE-Q) global scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. A global EDE-Q score at or above 2.8 indicate clinically significant ED pathology. Minimum score = 0, Maximum score = 6.0. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 3
Eating disorder examination questionnaire (EDE-Q) subscale scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. Minimum score = 0, Maximum score = 6.0. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 4
Patient health questionnaire (PHQ-9) scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. PHQ-9 cut-off scores: 0–4: No depression, 5–9: Mild depression, 10–14: Moderate depression, 15–19: Moderately severe depression, 20–27: Severe depression. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 5
Generalized anxiety disorder questionnaire (GAD-7) scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. GAD-7 cut-off scores: 0–4: No anxiety, 5–9: Mild anxiety, 10–14: Moderate anxiety, 15–21: Severe anxiety. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 6
Acceptance and action questionnaire v.2 (AAQ-II) scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. A score of 25 or higher reflects significantly reduced psychological flexibility, often associated with symptomatic presentations. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 7
EuroQol five dimension-five level (EQ-5D-5 L) health state scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. 0: Worst imaginable health state, 100: Best imaginable health state. The blue dots and lines represent KAP and ketamine booster sessions
Fig. 8
Ketamine side effect screening tool (KSET) scores across the 9-month assessment period. Note: KAP = Ketamine-assisted psychotherapy; Ket-Boost = Ketamine booster dose; SR = Self-report. 0: No side effects, 45: Overall severe side effects. The blue dots and lines represent KAP and ketamine booster sessions
Ketamine tolerability, adverse and unanticipated eventsVitals, including blood pressure, pulse, oxygen saturation, and respiratory rate, were recorded shortly before and after each ketamine session. The patient tolerated the treatments well, with no significant complications. During the second session, when the dose was first increased to 0.75 mg/kg, she experienced nausea and vomited once after 10 min, accompanied by a brief vagal response. This resolved within minutes. After the session, she was administered sublingual ondansetron for nausea, and the dose was reduced to 0.6 mg/kg for the subsequent treatment. Common post-ketamine side effects were reported including temporary dizziness, nausea, blurred vision, fatigue, and headache. No other adverse or unanticipated events occurred.
Subjective ketamine experiences and therapeutic outcomesDuring the ketamine treatments, the patient experienced a range of sensations and emotional responses. Initially, sensory experiences were minimal; she described being in a black room with grey, concrete-like stripes, briefly feeling dissociated, as if her head were large and her body small. This unfamiliar sensation dissipated quickly, leaving her feeling calm, connected to the music, and relaxed, with positive emotions. Over time, the experiences deepened, incorporating physical sensations such as floating, being tilted upside down, and feeling as though she were in a dark room or a serene natural setting, such as a forest or an ocean. The sessions increasingly evoked feelings of calm, connection, and love, sometimes accompanied by a profound emotional resonance with the music. The therapy sessions provided space to explore ED related struggles. The patient expressed a persistent preoccupation with weight loss, identifying an ideal weight she believed would enable her to achieve fulfilling relationships, career satisfaction, and family goals. Despite recognizing these thoughts as part of her illness, she expressed ambivalence about relinquishing them. Discussions centred on her desire for a future free from the constraints of her ED, highlighting the tension between her hopes for recovery and the entrenched beliefs about weight control. Throughout the treatment process, her emotional responses began to shift. She reported feeling calmer, more relaxed, and more connected to her emotions, particularly feelings of love and hope. At times, her mood remained sensitive to thoughts about her body, yet she also noticed moments of acceptance, describing her body as “okay” and a better space to “be in.” She observed significant improvements in her overall well-being, including increased energy, vitality, and the ability to engage in meaningful activities such as jogging and social interactions. Importantly, she became more open with her mother, sharing her struggles for the first time, which led to improved familial interactions and a sense of emotional relief. During treatment, the patient mentioned an instance where her brother-in-law visited and prepared meals for her and her sister. She reported experiencing heightened sensory awareness, particularly stronger perceptions of smell and taste, which she described as pleasurable and encouraging. By the end of the treatment series, the patient reported noticeable progress in both her physical and emotional states. She experienced a sense of lightness, even without changes in weight, and found calm in avoiding the scale—a previously distressing trigger. The sessions enabled her to imagine a future in which she could live without the ED, fostering motivation and hope for continued recovery.
Comments (0)