The true incidence of very rare complications associated with colonoscopy is difficult to determine even in high volume endoscopy centers. In contrast, data from registries probably give more reliable results. However, registries with a sufficient number of procedures are predominantly administrative data bases which allow only limited access to individual health reports of the patients. On the other hand, administrative data bases offer the big advantage of non-biased patient selection. Thus, studies relying on such large registries, e.g., of health insurance companies, reflect real-world data. Since the health insurance data base used in this study covers about 13% of the German population, the results probably come close to the general population for Germany.
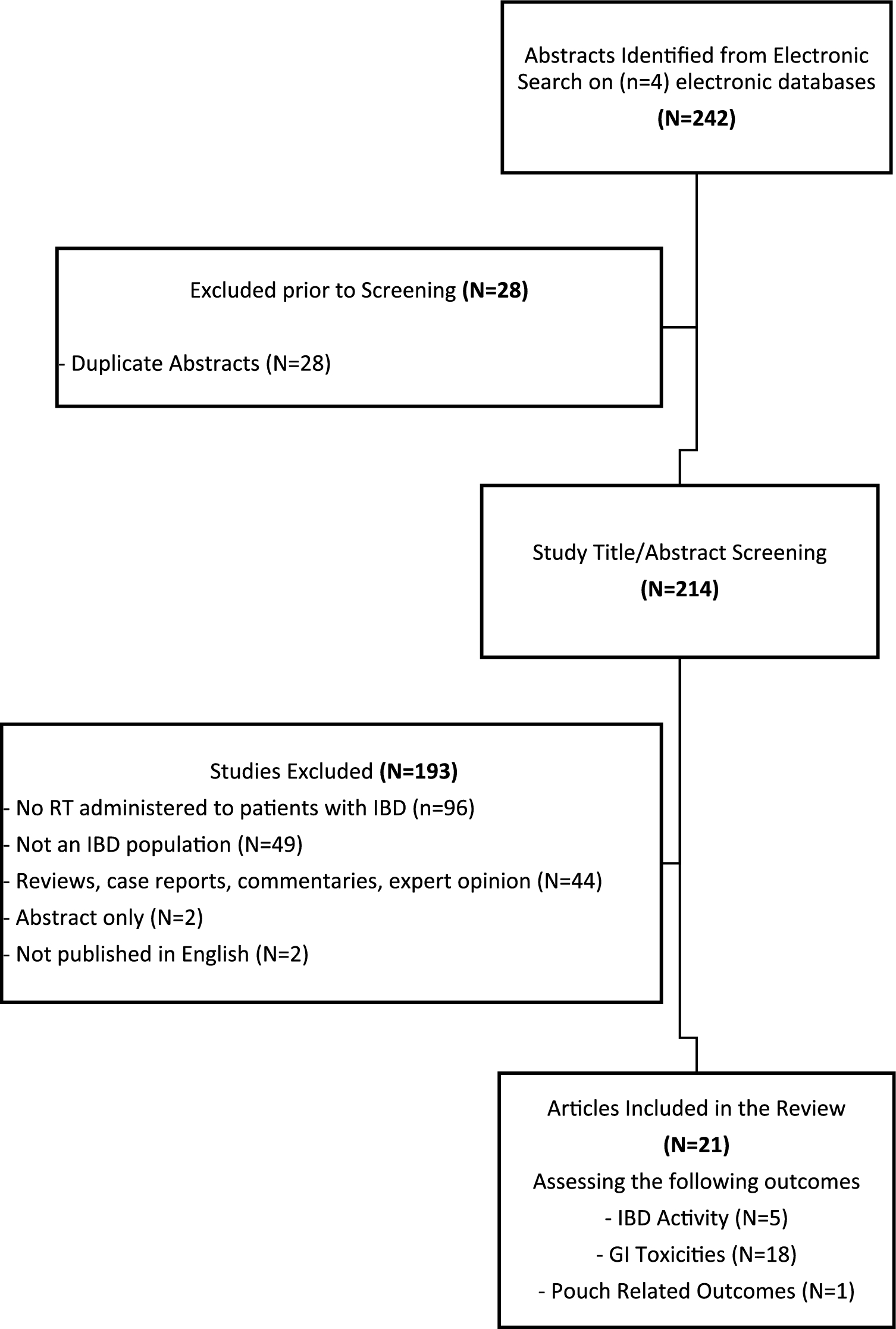
In the present study, data from about 1.6 million colonoscopies were analyzed in respect to the occurrence of splenic injuries. Results in 1.44 million out-patient colonoscopies are presented here. Previous studies on this rare complication in large out-patient cohorts give only limited insight since these investigations were focused on other parameters. Data on the time course, therapy and outcome were therefore very limited.
The study protocol of the present investigation used a broad spectrum of codes to capture all possible cases with post-colonoscopy splenic injuries. However, this protocol required a “safety feature” to avoid false allocation of cases popping up in the selection process who would eventually be misinterpreted as splenic injuries due to colonoscopy. Therefore, each case with an ICD code of a splenic lesion and an abdominal imaging or splenic surgery within the interval of 7 days from the date of colonoscopy was individually analyzed by a gastroenterologist and (in some cases) additionally by an experienced surgeon to exclude other mechanisms which may have led to the splenic insult. The individual reconstruction of the clinical course enabled to identify causes for splenic lesions and/or splenic surgery other than colonoscopy as, e.g., trauma and splenectomy for hemolytic anemia. Furthermore, in patients with additional abdominal surgery during the 7-day interval after endoscopy, e.g., because of colorectal, gastric, and pancreatic cancer, splenic injuries were attributed to surgery rather than colonoscopy due to the much greater probability of intraoperative iatrogenic splenic lesions [11]. Nevertheless, the study is based on administrative data, and results are thus depending upon the quality of coding. Inadequate coding cannot be completely excluded in every patient even despite a thorough individual case analysis.
Acknowledging the limitations of the study, there is clear evidence that out-patients have a significantly lower risk suffering from splenic injuries than hospitalized patients undergoing colonoscopy [3,4,5,6]. In the cohort of about 1.44 million out-patient colonoscopies the overall incidence accounts for 1 splenic injury per 31,400 endoscopies. This agrees to previous reports showing incidences between 1 case in 14,000 to 30,000 colonoscopies [7,8,9]. The reason for this distinct difference in the incidence is largely unknown, but hospitalized patients are older and more likely to suffer from various concomitant diseases, whereas out-patients are probably healthier. Age and concomitant disease are well established risk factors for complications of colonoscopy in general [9], and the relatively high incidence of splenic lesions in octogenarians [4] may indicate that this may also apply to splenic injuries.
There is still a debate about other relevant risk factors for splenic complications due to colonoscopy [12]. Previous surgery, excess traction upon the splenocolic ligament, pressure on the abdominal wall during endoscopy, and difficult passage of the colon have been discussed, but none of these hypotheses have been proven yet [13]. However, there is overwhelming evidence for a female preponderance in respect of splenic injuries [3, 4, 6, 14, 15]. It may be speculated that gender-specific anatomical differences also play a role: in males the splenic flexure is one vertebra higher and further from the midline in supine position compared to women [16]; however, the relevance of this anatomical difference remains open. According to Laanani [9], the qualification of the endoscopist is another risk factor for overall complications due to colonoscopy, and this may also apply to the subset of patients with splenic injuries. In Germany, gastroenterologists performing out-patient colonoscopy have to comply annually with rigid quality assurance requirements for reimbursement [17] which may have contributed to the relative low incidence of splenic injuries.
Two thirds of splenic injuries and particularly the more severe cases manifested within 48 h after the endoscopy but lesions necessitating surgery occurred even up to 6 days after colonoscopy. Therefore, the conclusion that 80% of cases are to be expected within 24 h [18] must be seriously questioned. CT scans were the overwhelming diagnostic procedure in the early phase after colonoscopy, whereas in the later course diagnoses were increasingly made by ultrasound investigation. The substantial role of ultrasound diagnoses may be surprisingly high but in Germany abdominal ultrasound is available in practically every gastroenterological unit.
Surgical treatment was performed in 41% of cases. Though operative therapy rates vary considerably up to 80% [2, 3, 11, 13, 15, 19], they are at least beyond 30% in most studies. Necessity for intensive care therapy and particularly transfusion requirements were strong predictors for the need of surgery. In accordance with previous studies [19, 20], the predominant operative procedure was splenectomy but a spleen-preserving surgical approach proved successful in some cases. In the study presented here, the fraction of patients with successful conservative management (59%) was relatively large compared to previous studies; different selection criteria may be responsible for the divergent results. Furthermore, conservatively managed lesions are probably underreported. Nevertheless, a recent trend toward an increase of conservative management has also been observed by Jahangir [2]. Prospective studies may fill the gaps of knowledge but are very difficult to perform.
In the view of the large number of colonoscopies performed (in Germany about 2 million per year) splenic injuries due to colonoscopy are relevant to physicians even beyond gastroenterologists. Naturally, every endoscopist should be aware of this complication, and patients should be informed about this—though rare—event. However, also family physicians may be confronted with delayed manifestations of this complication even several days after colonoscopy: the presence of the Kehr’s sign (left shoulder pain) in combination with upper left abdominal pain may guide to the diagnosis and appropriate management [21]. Symptoms occurring early after colonoscopy and compatible with a suspected splenic injury should be regarded as possibly life-threatening and should prompt immediate diagnostic imaging (preferentially CT scan).





Comments (0)