
Remember me




The new FIGO 2023 staging [1] for endometrial cancer (EC) includes various histological types, tumor patterns, and molecular classification [2], as they affect prognosis and enable a more appropriate treatment planning [3].
New histopathological variables included in the 2023 FIGO staging for EC:
Two histological types [4]:
Non-aggressive tumors: low-grade endometrioid carcinoma (grades G1 and G2).
Aggressive tumors: high-grade endometrioid carcinoma (grade G3) and non-endometrioid carcinoma (including serous, clear cell, undifferentiated, mixed, mesonephric-like, gastrointestinal-type mucinous carcinomas, and carcinosarcomas).
Incorporation of molecular subtypes [5]:
POLE mutation (associated with favorable prognosis).
p53 mutation (associated with poor prognosis).
The integration of molecular classification (POLE, p53, MMRd, NSMP) in the 2023 FIGO staging system reflects prognostic categories established through tissue-based analysis. MRI findings alone are not sufficient to determine these subtypes; however, certain imaging features—such as large heterogeneous masses, deep myometrial invasion, or lymph node involvement—may raise suspicion for aggressive behavior, particularly in p53-abnormal tumors. In clinical practice, molecular data are increasingly available preoperatively through endometrial biopsy and are used in conjunction with MRI findings to guide staging and management decisions.
Lymphovascular space invasion (LVSI) [6]:
Substantial LVSI is defined as involvement of five or more vessels, according to recent guidelines and pathological consensus [6]. This threshold holds prognostic value, as substantial LVSI is a well-established risk factor for metastases and recurrence in endometrial carcinoma, particularly in non-aggressive histological types and in early-stage endometrial carcinoma. Conversely, no LVSI or focal LVSI (less than 5 vessels involved) have been associated with significantly better prognostic outcomes. In the FIGO 2023 system, the presence of substantial LVSI may lead to upstaging to Stage IIB, even in tumors with otherwise favorable features.
While MRI cannot directly assess LVSI, certain imaging features may raise suspicion, such as irregular or spiculated tumor margins, disruption of the junctional zone, or ill-defined tumor-myometrium interfaces. Nevertheless, more studies should be done in order to define all the radiological spectrum of the substantial or focal linfovascular invasion. Awareness of histological LVSI status is crucial when interpreting MRI for staging and treatment planning.
This review summarizes the updates in the FIGO 2023 staging, emphasizing the differences compared to the FIGO 2009 system. It also correlates MRI findings with the updated staging and highlights imaging data crucial for managing patients with EC [7, 8].
Changes between the 2009 and 2023 FIGO staging systems for EC (Table 1).Stage IA subdivided into:
IA1: no myometrial invasion (non-aggressive EC).
IA2: myometrial invasion < 50% (non-aggressive EC).
IA3: ovarian involvement and myometrial invasion < 50% (non-aggressive EC).
Stage IC: aggressive histological types limited to an endometrial polyp or confined to the endometrium.
Stage II subdivided into:
Stage IIIA subdivided into:
Stage IIIB subdivided into:
Stage IIIC subdivided into:
IIIC1: pelvic lymph nodes.
IIIC2: infrarenal para-aortic lymph nodes.
Each with micrometastasis (i) or macrometastasis (ii).
Stage IVB subdivided into:
IVB: peritoneal metastases beyond the pelvis.
IVC: distant metastases, including inguinal and intra-abdominal lymph nodes above the renal vessels.
Table 1 Changes in FIGO staging for endometrial cancer (EC)Implications of the 2023 FIGO Staging of EC in MRI: MRI plays a key role in identifying prognostic factors preoperatively:
Stage I Myometrial invasion.
Stage II Cervical stroma invasion.
Stage III: ovarian/fallopian involvement, uterine subserosal involvement, vaginal/parametrial invasion, peritoneal spread, pelvic/para-aortic lymph node metastasis.
Stage IV: bladder or intestinal mucosal invasion, distant metastasis.
2023 FIGO stage ICombination of histologic findings and presence and depth of myometrial invasion. Includes tumors confined to the uterine corpus; without LVSI; with a non-aggressive histological type (with or without myometrial invasion), or any aggressive histological type confined to the endometrium (no myometrial invasion).
IA1 Non-aggressive, no LVSI, in an endometrial polyp or confined to the endometrium.
IA2 Non-aggressive, no LVSI, myometrial invasion < 50%.
IA3 Non-aggressive, no LVSI, myometrial invasion < 50%, ovary involvement.
IB Non-aggressive, no LVSI, myometrial invasion ≥ 50%.
IC Aggressive histological types limited to an endometrial polyp or confined to the endometrium.
In the revised FIGO 2023 cancer staging, histologically non-aggressive tumors limited to an endometrial polyp are classified as Stage IA1 (previous FIGO staging was Stage IA) (Fig. 1). It is important to confirm/exclude myometrial invasion, as it is an essential prognostic risk factor [9, 10].
Fig. 1
Stage IA1 grade 1 endometrioid carcinoma, no LVSI, in a 48-year-old woman. A Axial oblique T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms, slice thickness 3 mm) and B contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show an endometrial polyp without myometrial invasion (arrow). On the T2-WI, hyperintense cystic spaces are seen within the polyp (arrowhead)
Low-grade endometrial carcinoma extending < 50% into the myometrium are classified as Stage IA2 (previously Stage IA)(Fig. 2). Disruption of the junctional zone in uterine fundus is better appreciated on contrast-enhanced T1-weighted fat-saturated MR images [11].
Fig. 2
Stage IA2 grade 2 endometrioid carcinoma, no LVSI, and myometrial invasion < 50% in a 58-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show an endometrial mass with superficial myometrial invasion (arrows)
Low-grade endometrial carcinoma involving both endometrium and ovary, and meeting specific criteria are classified as Stage IA3 (previously Stage IIIA) (Fig. 3). These must be distinguished from extensive EC spread to the ovary (Stage IIIA1) by the following criteria:
1.No more than superficial myometrial invasion (< 50%).
2.Absence of LVSI.
3.Absence of additional metastases.
4.Unilateral ovarian tumor, confined to the ovary, without capsule invasion/rupture (pT1a).
Patients with low-grade endometrioid carcinomas limited to the uterus and the ovaries are considered to have a good prognosis and no adjuvant treatment is recommended [3].
Fig. 3
Stage IA3 grade 2 endometrioid carcinoma, no LVSI, confined to the endometrium and left ovary in a 60-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) shows a mass confined to the endometrium without myometrial invasion (arrow). B Axial T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and (C diffusion-weighted image (DWI) with b = 800 s/mm2 show a nodule in the left ovary without capsule invasion (arroweads). Cysts in the right ovary (chevron). Pathology confirmed low grade endometrial carcinoma involving both endometrium and left ovary
Low-grade endometrial carcinomas which extend more than 50% into the myometrium are classified as Stage IB (unchanged from previous staging) (Fig. 4). When the tumor exceeds 50% into the myometrium, the presence of an intact stripe of normal outer myometrium excludes uterine serosa invasion [12, 13].
Fig. 4
Stage IB grade 2 endometrioid carcinoma, no LVSI in a 60-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B axial oblique T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) show an endometrial mass with myometrial invasion (arrows). C Axial contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) shows disruption of the junctional zone. Pathology confirmed low grade endometrioid carcinoma involving > 50% of the myometrium
Any aggressive histological type without myometrial involvement is Stage IC (previously Stage IA) (Fig. 5). The risk of extrauterine disease in aggressive endometrial carcinomas does not correlate with the depth of myometrial invasion as nodal or intraperitoneal metastases can occur even when there is no myometrial invasion [14].
Fig. 5
Stage IC carcinosarcoma, no LVSI in a 67-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B Sagittal contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 3 min) show a bulky endometrial tumor distending the endometrial cavity without myometrial invasion. Preservation of the junctional zone is better appreciated on dynamic images after contrast (arrow). Pathology confirmed carcinosarcoma limited to the endometrium
Tips for MRI interpretation: stage IIt is important to confirm or exclude myometrial invasion, as it is a key prognostic risk factor.
The depth of myometrial invasion is best measured on axial oblique images perpendicular to the endometrial cavity.
The extent of myometrial infiltration by carcinoma is categorized as: none; <50%; or ≥ 50%.
Dynamic multiphase contrast-enhanced imaging (DCE) improves the accuracy of assessing myometrial invasion by demonstrating a smooth, uninterrupted band of subendometrial enhancement and helping to exclude superficial myometrial invasion.
2023 FIGO stage IICombination of histological findings, myometrial invasion and cervical stroma invasion.
Includes cervical stroma invasion in non-aggressive histological types without extrauterine extension, non-aggressive histological types with substantial LVSI, or aggressive histological types with myometrial invasion.
IIA Cervical stroma invasion in non-aggressive tumors with no LVSI.
IIB Substantial LVSI in non-aggressive histological types.
IIC Aggressive histological type with any myometrial invasion.
In the revised FIGO 2023 endometrial cancer staging, non-aggressive histological tumors without extrauterine extension are classified as Stage IIA (previously Stage II) (Fig. 6). Disruption of the cervical stroma is better appreciated on delayed contrast-enhanced T1-weighted fat-saturated MR images [12, 15].
Fig. 6
Stage IIA grade 2 endometrioid carcinoma, no LVSI, in a 65-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B sagittal contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show disruption of the junctional zone (arrow). The tumor extends more than 50% into the myometrium and into the cervical canal with disruption of the cervical stroma (arrowheads), best seen on delayed phase images
Aggressive histological tumors with any myometrial involvement are classified as Stage IIC (previously Stage IB) (Fig. 7). This change reflects evidence from randomized trials, prospective cohort studies, large database series, and retrospective reports that consistently show aggressive histological types have a markedly higher recurrence rate [16, 17].
Fig. 7
Stage IIC carcinosarcoma, no LVSI in a 67-year-old woman. A Axial oblique T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B a contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show a mass invading the superficial myometrium and a peripheral rim of normally enhancing myometrium (arrow)
Tips for MRI interpretation: stage IIAssessment of cervical stroma invasion best depicted on delayed images after intravenous gadolinium administration.
Suspect cervical stroma invasion when the cervical mucosa enhancement is disrupted by a poorly enhancing tumor on delayed images (4–5 min after contrast).
Continuous enhancement of the cervical mucosa on delayed phase images excludes cervical stroma invasion.
Distinguish between tumor protruding from the endometrial cavity into the endocervix (stage I), and cervical stroma invasion (stage II).
2023 FIGO stage IIIIncludes local and/or regional spread of the tumor of any histological type.
IIIA: Direct or metastatic invasion of uterine serosa, adnexa, or both.
IIIB: Direct or metastatic invasion of the vagina and/or parametria or pelvic peritoneum.
IIIC: Metastasis to pelvic or para-aortic lymph nodes or both.
IIIC1: Metastasis to pelvic lymph nodes.
IIIC2: Metastasis in infrarenal para-aortic lymph nodes with or without pelvic lymph node metastasis.
In the revised FIGO 2023 endometrial cancer staging, any histological subtype with ovarian metastasis is classified as Stage IIIA1 (previously Stage IIIA) (Fig. 8). Spread of the EC to the ovary (Stage IIIA1) must be distinguished from low-grade EC involving < 50% myometrium and ovaries (Stage IA3). Patients with extensive spread of the EC to the ovary (Stage IIIA1) have a worse prognosis, and adjuvant treatment is recommended [18,19,20].
Fig. 8
Stage IIIA1 grade 3 endometrioid carcinoma, in a 70-year-old woman. A Sagittal and B axial T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and C) axial contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show a large endometrial mass distending the uterine cavity with myometrial invasion, extending into the cervical channel with stromal invasion. On axial T2WI and on dynamic contrast-enhanced images a right parauterine heterogeneous mass is demonstrated (arrows). Right ovarian metastasis was confirmed by pathology
Any histological subtype with direct adnexal extension is also classified as Stage IIIA1 (previously Stage IIIA) (Fig. 9). Subclassifications of Stage III were defined to better reflect tumor behavior, especially in high-grade and non-endometrioid carcinomas [21].
Fig. 9
Stage IIIA1 carcinosarcoma in a 72-year-old woman. A T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B axial contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show absent myometrial signal intensity and a right adnexal mass (arrow). Pathology confirmed involvement of the myometrium and right adnexa by carcinosarcoma
Uterine serosa infiltration is classified as Stage IIIA2 (previously Stage IIIA) (Fig. 10). The subclassification of Stage III aims to better reflect prognosis and support more appropriate treatment decisions [1].
Fig. 10
Stage IIIA2 serous carcinoma in a 70-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) and B sagittal contrast-enhanced 3D T1-weighted fat-suppressed LAVA sequence (TR/TE: 4.2/2.1 ms; slice thickness: 2 mm; post-gadolinium, delayed phase at 4 min) show absent normal myometrial signal intensity and an irregular uterine contour at the fundus (arrows). Pathology confirmed serous carcinoma with involvement of the uterine serosa
Pelvic peritoneal metastases are now classified as Stage IIIB2, distinct from peritoneal involvement that extends beyond the pelvis, which is classified as Stage IVB (Fig. 11). Treatment decisions vary significantly depending on whether peritoneal carcinomatosis is limited to the pelvis (Stage IIIB2) or extends beyond (Stage IVB). The anatomical landmark of the pelvis is the line between the anterior superior iliac spines [22].
Fig. 11
Stage IIIB2 uterine serous carcinoma in a 70-year-old woman. A Sagittal T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm), B axial diffusion-weighted image (DWI) with b = 1000 s/mm2, and C ADC map show a uterine mass (arrow) and peritoneal implants in the Douglas pouch (arrowheads). ADC value in the peritoneal implant is 0.65 × 10−3 mm2/s
Metastasis to para-aortic lymph nodes up to the renal vessels is classified as Stage IIIC2, distinct from intra-abdominal or para-aortic lymph nodes above the renal vessels, which are classified as Stage IVC (Fig. 12). Staging distinguishes para-aortic lymph nodes as Stage III vs. Stage IV using the renal vessels as the boundary. Lymph node metastases alter prognosis and modify the therapeutic approach [23].
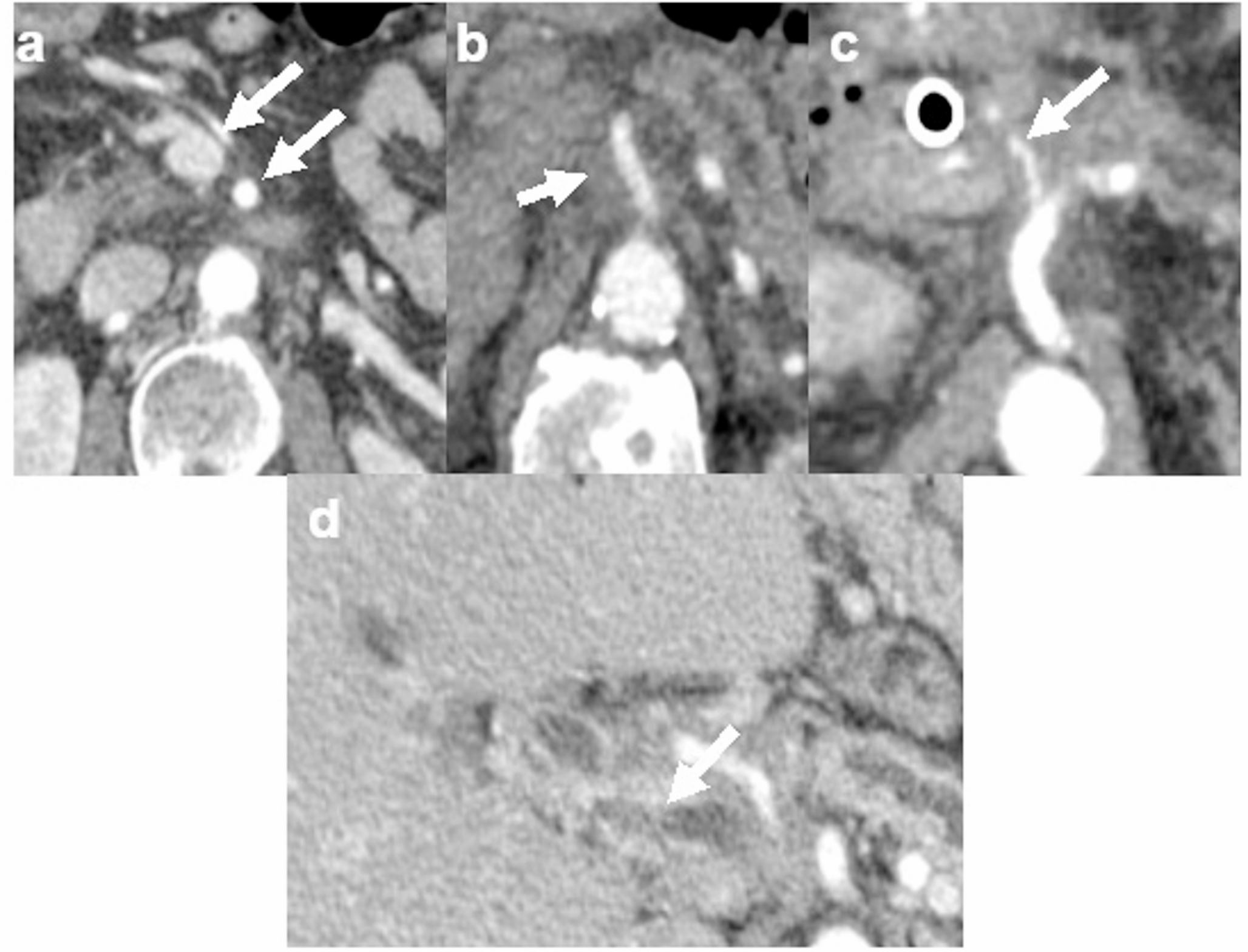
Fig. 12
Stage IIIC2 grade 2 endometrioid carcinoma in a 63-year-old woman. A Axial fat-suppressed T2-weighted fast spin-echo (FSE) image (TR/TE: 4500/100 ms; slice thickness: 3 mm) shows an enlarged para-aortic lymph node (arrow). B Axial diffusion-weighted image (DWI) with b = 800 s/mm2 shows a hyperintense lymph node (arrow). ADC value in the node is 0.94 × 10−3 mm2/s. Pathological analysis confirmed lymph node metastases
Comments (0)