
Remember me




This single-center, retrospective study protocol was approved by the Ethics Committee of the Fifth Medical Center of the Chinese PLA General Hospital (Beijing, China) and was conducted in accordance with the principles of the Declaration of Helsinki. From October 2020 to December 2023, a cohort of 30 patients who underwent ultrasound-guided percutaneous microwave ablation (US-PMWA) with the aid of a 3D visualization operative planning system were enrolled in the study. A separate cohort of 60 patients who underwent US-PMWA using conventional 2D image operative planning methods served as controls. Data from the patients were extracted from our maintained registry database (ratification no. 20100930-004, registration no. ChiCTR-TRC-10001119). These patients were matched for lesion volume and lesion location. The inclusion criteria for US-PMWA were as follows: (1) a single uterine fibroid (≥ 5 cm) diagnosed by MRI and ultrasound with a clinical syndrome such as menorrhagia and dysmenorrhea; (2) patients with no plans for future pregnancy; (3) US-PMWA not combined with other treatments such as ethanol injection; and (4) patients with MRI examinations within 7 days before and after US-PMWA. The exclusion criteria included the coexistence of other pelvic or uterine diseases (e.g., pelvic inflammatory diseases, ovarian endometriomas, or uterine adenomyosis) or previous treatment such as uterine artery embolization, radiofrequency ablation (RFA), or high-intensity focused ultrasound.
3D visualization operative planning systemAll patients with uterine fibroids underwent MRI to delineate the target lesion within 3 days before ablation. A desktop computer (Lenovo) with an Intel Core i5 processor was used for an empirical study in our department to perform 3D visualization preoperative planning. A series of MRI data (0.625 mm- or 2.5 mm-thick slices) of the lesion before ablation were converted to DICOM format and then imported into the 3D visualization treatment platform (Hokai Company, Zhuhai, China). The 3D visualization platform used in this study was a research prototype developed by Ping Liang (Hokai Company, Zhuhai, China) during the trial period (2020–2023). It has since undergone CE certification and commercialization as part of ongoing technology transfer efforts. The current commercial version retains the core functionalities described herein.
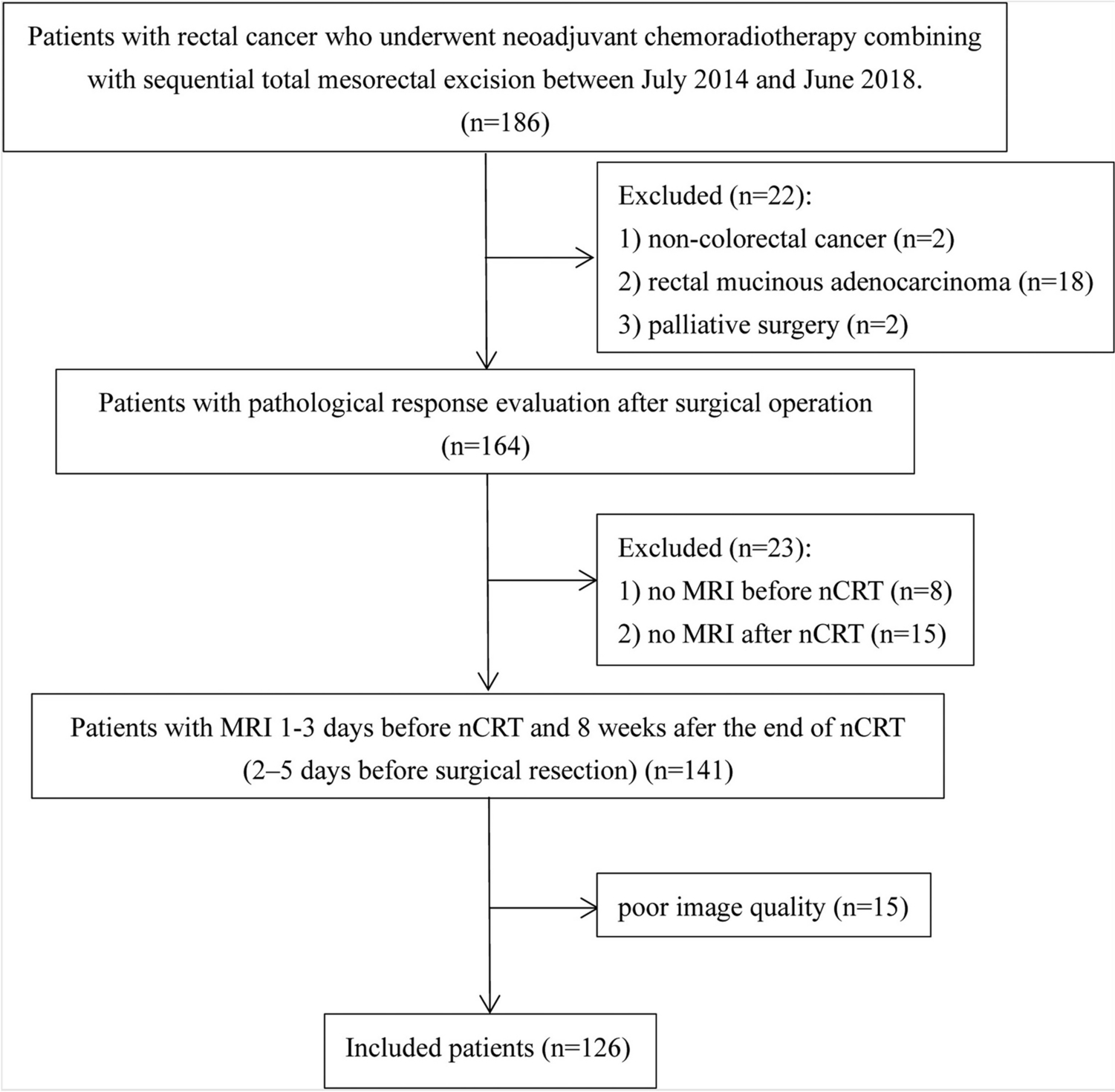
Our group (PingLiang) originally developed the 3D visualization platform software, which has novel functions as follows: (1) rapid segmentation of the target (within 2 min); (2) volume calculation of the target; (3) simulation of the thermal field; (4) interactive pre-ablative planned strategy by manual operation; and (5) assessment of ablative effect by tumor mapping (Fig. 1). The graphical user interface displayed the real-time simulation 2D ultrasound-guided planning and the 3D visualization planning, as well as the planning path from the transverse, coronal, and sagittal planes. The application of 3D visualization technology enables a radiologist to perform various operations on the 3D image, such as free movement, rotation, and scaling, to develop a puncture plan by seeing more intuitively. The myoma with a 5-mm margin, endometrium, and surrounding vital structures were segmented and reconstructed, which can be demonstrated via stereo display in the 3D visualization (Fig. 1).
Fig. 1
A MRI was performed before microwave ablation for each patient (slice thickness less than 0.5 mm); B The MRI with DICOM format data of 3D group patients was transformed into a 3D visualisation preoperative planning system for processing and analysis.(Yellow: uterus;green:lesion;red:uterine endometrium white:bladder black:intestinal tract);C 3D visualization operative planning system showed the location and relationship with the lesion and the surrounding organs and the quantitative distance between the lesion and surrounding vital structures were acquired (Dark pink silhouette:uterus; dark yellow and bright yellow:lesions; red:uterine endometrium blue:bladder;Dark gray:rectum;light gray:spine); D, E The volume of the lesion and uterus was quantized by the operative planning system and microwave ablation power and action time were calculated according to the dose–effect relationship of microwave ablation. Then 3D visualization operative planning system projected the number and the pathway of the ablation antenna implantation, the ablation time and energy, simulated the thermal field, and provided the location of the aspiration. The 3D planning system simulated 13 overlapping ablation zones in this case (D represented one ablation zone) to ensure complete fibroid coverage. Two percutaneous punctures were made, and the antenna were repositioned 11 times along predefined intralesional trajectories (E) to replicate the simulated thermal fields. F In the MRI image 3 m after ablation, the lesion residual nuclear and ablation zones were clearly demonstrated and the NPV ratio was calculated.
The 3D operation planning system of US-PMWA should adhere to the following principles: (1) avoid ablation of the bladder, ovary, and intestinal tract, particularly the endometrium; (2) minimize the number of antenna insertions and ablation points; and (3) minimize the distance of antenna insertion trajectories while avoiding puncture pathways through critical structures. The planning system was designed to iterate these goals until a reasonable and feasible plan was achieved [14] (Fig. 1).
US-PMWAA cooled-shaft MW tumor coagulator (KY-2000; Kangyou Medical, Nanjing, China) consisting of a 15-gauge needle antenna with a 1.1 cm exposed tip was used. This microwave ablation tumor coagulator can produce 100W of power at 2450 MHz. A power output between 40 and 60W was used during ablation. The antenna was percutaneously inserted into the lesion under the guidance of transabdominal ultrasound. The entire ablation procedure was performed under real-time US guidance [1]. Proper microwave ablation power and ablation time were chosen according to the preoperative plan of the 3DVOPS. The antennae were inserted into the location of the lesion according to the 3DVOPS. The hyperechoic area of ablation was monitored by real-time greyscale ultrasound, and the end of ablation was determined when the hyperechoic coverage of the proposed ablation area. The effectiveness of ablation was then immediately assessed using contrast-enhanced ultrasonography (CEUS, SonoVue, Bracco SinePharm, Milan, Italy). Nonenhanced regions on CEUS indicated necrotic areas.
Assessment of technical efficacy and safetyFor the technical efficacy evaluation, the ablation time, ablation energy, non-perfused volume (NPV), and NPV ratio were assessed. The ablation energy was calculated as ablation power × ablation time. The extent of the NPV was evaluated by enhanced MRI performed within 3 days after the ablation. The NPV and lesion volume were calculated as 0.5233 × superoinferior diameter × anteroposterior diameter × transverse diameter. The NPV ratio was calculated by the following equation: NPV ratio = (Necrotic tissue volume/lesion volume) × 100%. For the evaluation of safety, MRI was performed within 3 days after the ablation to evaluate the injury to the surrounding organs. The complications were classified according to the unified standardized Society of Interventional Radiology (SIR) grading system.
Statistical analysisData were analyzed using SPSS 21.0 for Windows (SPSS Inc., Chicago, IL, USA). The paired t-test or x2 test was used to compare values between the groups. The comparison of continuous variables between two groups was performed via Student’s t-test or the Mann–Whitney U-test. Pearson chi-squared analysis or Fisher exact tests were performed to compare the categorical variables. P values < 0.05 were considered statistically significant.
Comments (0)