
Remember me



During an index colonoscopy due to a positive family history, a broad-based adenoma was identified in the cecum of a 40-year-old male patient by an external endoscopist.
The clinical course and timeline of the case started with tumor removal in our hospital using endoscopic submucosal dissection (ESD). High-grade mucosal dysplasia and a transition to invasive adenocarcinoma were confirmed histologically. Subsequent preoperative staging did not indicate distant metastasis, leading to the recommendation of surgical treatment after discussion in the institution’s interdisciplinary tumor board.
A laparoscopic, oncological right hemicolectomy with CME and reconstruction with an ileotransverse laterolateral anastomosis was performed without initial complications. Vascular supply to the ileocolic artery and vein was managed near their respective origins from the superior mesenteric vessels at the lower edge of the pancreas using polymer clips (GRENA® Ligating Clips L purple; GRENA Ltd. Brentford, UK). The right colonic vessels were dissected during CME, and, due to their small caliber, ligated with a Ligasure® (Medtronic GmbH, 710 Medtronic Parkway, Minneapolis, MN 55432-5604 USA) device.
The final histopathological examination confirmed a moderately differentiated adenocarcinoma of the cecum, immunohistochemically microsatellite-stable, G2, pT2, pN1a (1/46), L0, V0, Pn0, R0 (UICC [Union Internationale Contre le Cancer] stage IIIA). The patient was discharged from the hospital in good overall condition.
Following discussion of his case in the interdisciplinary tumor board and due to nodal positivity, adjuvant combination chemotherapy with capecitabine and oxaliplatin (CAPOX) was initiated for four scheduled cycles over 3 months.
In the further course, the patient presented to our hospital twice due to abdominal pain and increased inflammatory parameters. The CT scan suggested microperforation of the laterolateral ileotransversostomy, necessitating hospitalization with intravenous antibiotics (piperacillin/tazobactam 3 × 4.5 g/day for 10 days). Conservative measures led to a rapid improvement of symptoms.
After receiving the third course of chemotherapy, another increase in infection parameters and abdominal pain occurred. Another CT scan was performed and showed an inflammatory retention between the anastomosis and the duodenum. After yet another course of antibiotics, the inflammatory parameters declined. Chemotherapy was terminated prematurely after the third cycle due to repeated inflammatory complications.
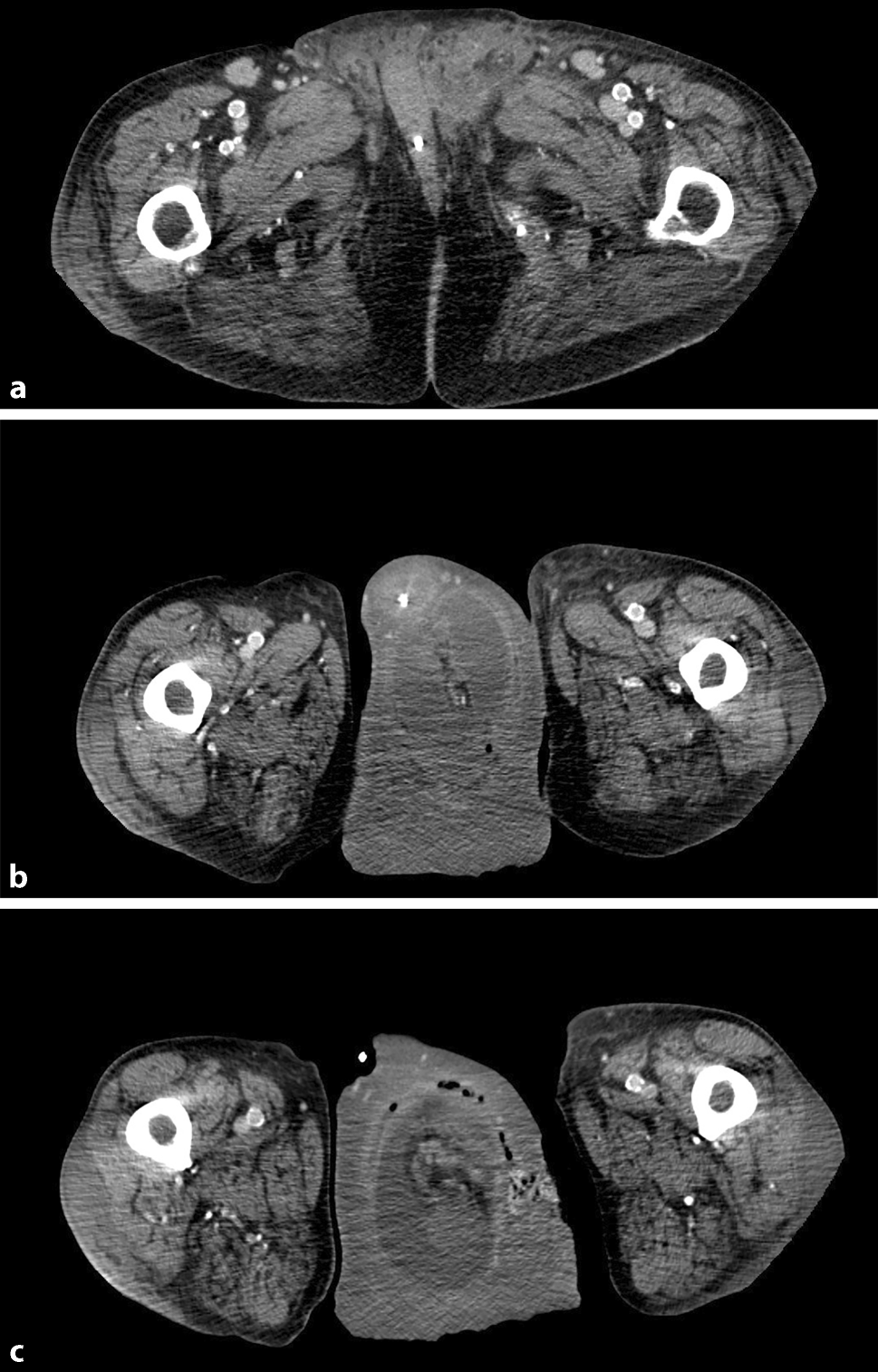
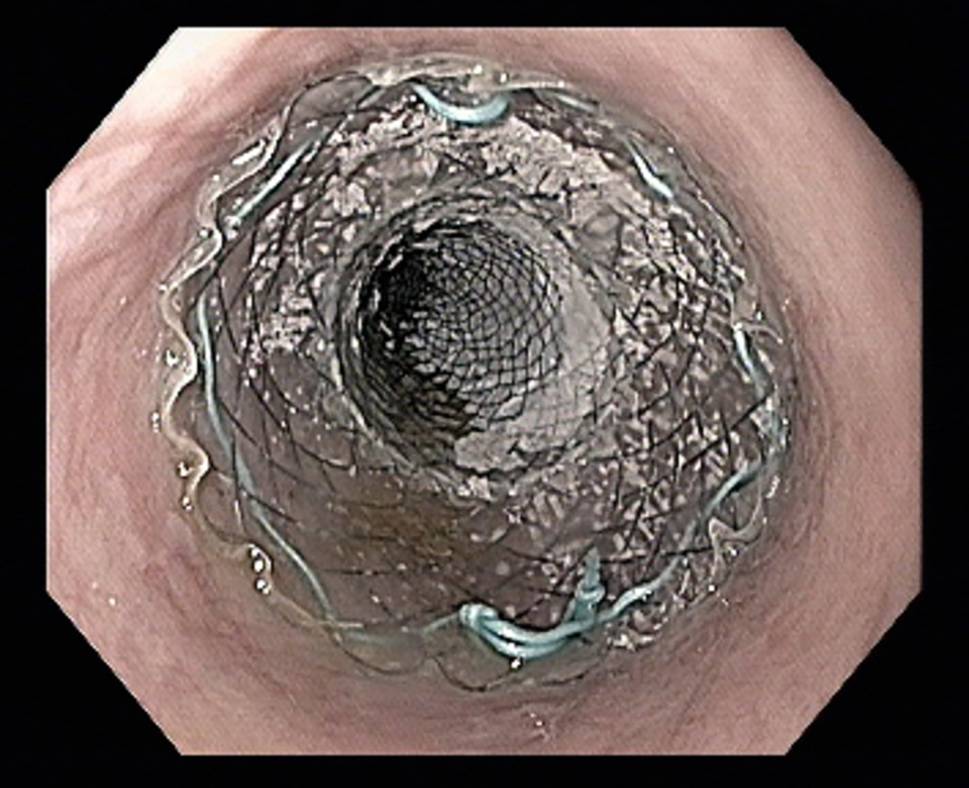
Seven months after the primary operation, the patient again presented to the emergency department with acute and severe abdominal pain. A CT scan (Fig. 1a) now confirmed a free hollow organ perforation with generalized peritonitis. Immediate surgical exploration was indicated. Preoperatively and already under general anesthesia, an esophagogastroduodenoscopy was performed, which revealing a GRENA® clip that had partially migrated into the duodenal lumen (Fig. 1b), causing an intraabdominal fistula from an abscess cavity to the duodenum.
Fig. 1
a Axial CT scan of the abdomen. Arrow showing free air in the abdominal cavity and signs of acute peritonitis. Arrowhead showing inflammatory process suggestive of abscess formation at the duodenum. b Gastroscopic view. Arrow showing the polymer clip protruding into the duodenum at the tip of endoscopic grasper
After subsequent median laparotomy, the clip was removed and an already evacuated abscess cavity between the duodenum and the anastomosis was found along with a small leak at the ileal stump. The fistula into the duodenum was confirmed in simultaneous esophagogastroduodenoscopy.
During surgery the ileocecal stump of the pre-existing anastomosis was shortened. The duodenal fistula was sutured with two rows of absorbable running suture. Due to concomitant adhesive small bowel obstruction with segmental stenosis formation, a small bowel resection was performed. Reconstruction was achieved with a laterolateral ileoileostomy.
The subsequent postoperative course was uneventful. Inflammatory parameters regressed under established intravenous antibiotic therapy, and oral intake of fluids and solid food was resumed. The patient was free of abdominal complaints and was discharged for oncological follow-up. To date, the patient remains free of recurrence or abdominal complaints.
Comments (0)