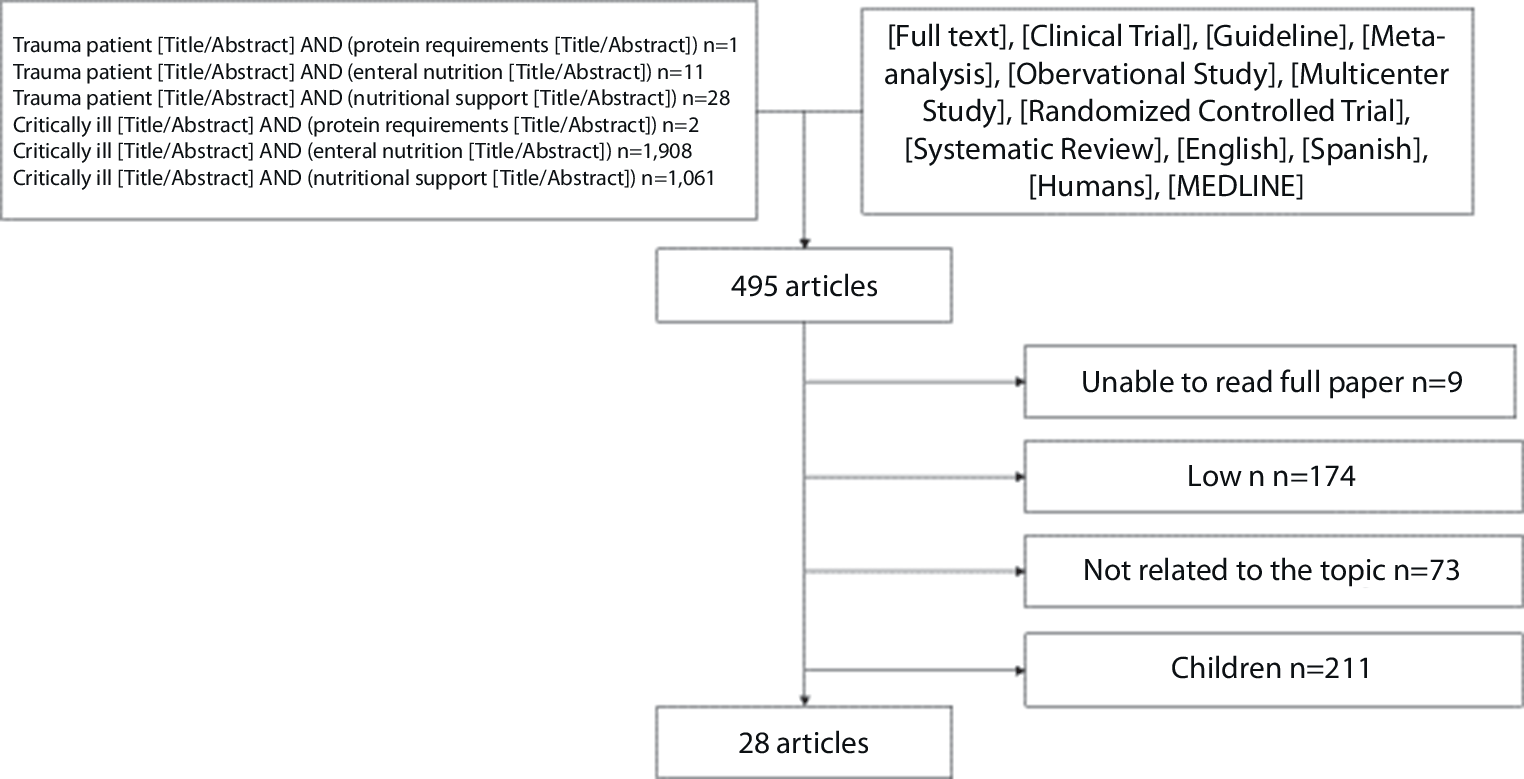
Out of 549 articles selected using the filters, 467 were excluded for the reasons outlined in Fig. 1.
The first step in diagnosing malnutrition is identifying patients who are malnourished or at risk of malnutrition. A general clinical assessment should be conducted to evaluate malnutrition in the intensive care unit (ICU), until a specific tool has been definitively validated ([6]; Table 1).
Table 1 Clinical assessment to assess malnutrition in the ICUNutritional support for trauma and critically ill patients must be tailored to the patient’s clinical phase, as metabolic demands and tolerance can vary significantly. The hyperacute phase focuses on hemodynamic stabilization, during which nutritional interventions are often postponed. In the acute phase, careful initiation of nutritional support is essential to prevent complications such as refeeding syndrome. During the recovery phase, prioritizing higher caloric and protein intake is crucial to meet the demands of healing and rehabilitation. These phases inform the strategies discussed in this review.
Energy expenditure and protein needs in trauma and critically ill patients
An accurate estimation (Table 1) of energy expenditure is essential for effective and optimal nutritional support in trauma and critically ill patients. Indirect calorimetry (IC) remains the gold standard for measuring resting energy expenditure (REE), allowing precise adjustments to caloric intake. However, IC is often unavailable in clinical settings due to cost and resource restrictions [1, 3].
Recent guidelines highlight the limitations of predictive equations, which frequently fail to account for the dynamic and heterogeneous metabolic states in critically ill and trauma patients [4, 7]. As an alternative, simplified caloric estimations, such as 20–25 kcal/kg/day for critically ill patients and 25–30 kcal/kg/day for trauma patients, have emerged as practical and reliable methods when IC is not available [8, 9]. These estimations strike a balance between underfeeding, which exacerbates malnutrition, and overfeeding, which is associated with complications such as hyperglycemia and hepatic steatosis [10].
Protein needs remain particularly elevated in both populations due to severe catabolism. Simplified recommendations suggest protein intake of 1.5–2.5 g/kg/day, depending on the severity of the injury or illness [2, 11]. Early initiation of high-protein enteral nutrition (EN) has demonstrated benefits in reducing nitrogen loss, preserving lean body mass, and promoting wound healing in trauma patients [2, 10].
Timing of nutritional support
The timing of nutritional support plays a pivotal role in patient outcomes. Early initiation of EN within the first 24–48 h after injury or ICU admission has been consistently associated with reduced sepsis rates, shorter ICU stays, and lower mortality [5, 12, 13]. Trauma patients undergoing resuscitation and critically ill patients with refractory shock require individualized timing based on hemodynamic stability to prevent exacerbating organ dysfunction [8, 14, 15].
Route of administration
The selection of the appropriate delivery method for nutritional support in trauma and critically ill patients depends on gastrointestinal function, metabolic needs, and the patient’s clinical condition and hemodynamic status. Enteral nutrition (EN) is the preferred approach whenever feasible due to its physiological benefits, which include maintaining gut integrity, reducing bacterial translocation, and minimizing infectious complications [4, 16].
Enteral nutrition can be administered via several routes, with nasogastric or orogastric feeding being most common for patients with intact gastric motility. These methods are simple, cost effective, and generally well tolerated. However, in trauma patients with a basilar skull fracture, an orogastric tube is preferred over a nasogastric tube to avoid complications such as intracranial placement through a disrupted cribriform plate [4, 9]. For patients with gastric dysmotility, aspiration risk, or severe trauma, post-pyloric feeding may be required. Feeding tubes can be advanced beyond the stomach and into the jejunum via nasojejunal or gastrojejunostomy routes, ensuring reliable nutrient delivery while reducing the complications associated with delayed gastric emptying [9].
Monitoring of gastric residual volumes (GRVs) is commonly employed to assess tolerance to EN, but its routine use remains controversial. Recent evidence suggests that clinical signs such as vomiting, abdominal distension, or diarrhea are more reliable indicators of intolerance than strict GRV thresholds [4, 16].
When EN is not feasible due to conditions such as bowel ischemia, ileus, or perforation, total parenteral nutrition (TPN) becomes necessary [4, 5]. Administration of TPN requires a central venous catheter (CVC) to safely deliver hyperosmolar nutrient solutions. Peripheral administration may be considered for short-term or less concentrated solutions, but central access is preferred for prolonged TPN to reduce the risk of vein irritation and ensure adequate nutrient delivery [4].
Total parenteral nutrition requires meticulous monitoring to prevent metabolic complications including hyperglycemia, hypertriglyceridemia, and liver dysfunction [10]. Additionally, the risk of catheter-related bloodstream infections necessitates strict aseptic techniques during catheter insertion and regular care to minimize infections.
In cases where EN alone is insufficient to meet the patient’s caloric requirements, a combined approach of EN and TPN can be used to optimize nutritional delivery while awaiting recovery of gastrointestinal function. This hybrid strategy ensures that energy and protein needs are met without over-relying on TPN, which may have a higher risk of complications [4, 17].
Tolerance to nutritional support
Ensuring tolerance to nutritional support is a critical aspect of care in trauma and critically ill patients, as intolerance can significantly compromise the delivery of adequate nutrition and increase the risk of complications. The approaches to managing tolerance differ depending on whether the patient is receiving enteral nutrition (EN) or total parenteral nutrition (TPN).
Enteral nutrition
Trauma patients, particularly those with abdominal or thoracic injuries, frequently experience delayed gastric emptying and gastrointestinal dysmotility due to their severe inflammatory and metabolic responses. In such cases, strategies like post-pyloric feeding via nasojejunal tubes or the use of prokinetic agents such as metoclopramide or erythromycin are effective for enhancing gastric motility and ensuring safe and adequate nutrient delivery. For patients unable to tolerate gastric feeding, jejunal feeding routes provide a reliable alternative for reducing the risk of aspiration and improving tolerance [9, 18, 19].
Monitoring clinical signs of intolerance, such as vomiting, abdominal distension, or diarrhea, remains a cornerstone of EN management. Evidence suggests that GRVs, traditionally used to assess feeding tolerance, are less reliable and should not be the sole parameter for decision-making. Current guidelines recommend focusing on clinical signs over strict GRV thresholds, as this approach minimizes unnecessary feeding interruptions and delays in achieving nutritional goals [4, 16]. Additionally, protocols to address interruptions caused by factors like sedation, prone positioning, or medical procedures can help ensure continuity of feeding and better overall tolerance [19].
Total parenteral nutrition
Total parenteral nutrition tolerance issues are primarily related to metabolic and infectious complications. Hyperglycemia, hypertriglyceridemia, and liver dysfunction are common challenges, requiring regular monitoring and timely adjustments to nutrient composition or infusion rates [14, 20]. Refeeding syndrome is a critical concern, especially in malnourished patients transitioning to TPN. To mitigate this risk, caloric intake should be increased gradually, with close monitoring of electrolytes such as phosphate, potassium, and magnesium to prevent life-threatening imbalances [21].
Infection control is another key consideration for TPN, as catheter-related bloodstream infections pose significant risks. Adherence to strict aseptic techniques during catheter insertion and maintenance, as well as routine monitoring for early signs of infection, is essential to reduce these complications [1, 22].
By addressing these challenges and tailoring interventions to each patient’s specific clinical needs, both EN and TPN can be optimized to maximize their benefits while minimizing associated risks.
Biochemical markers and metabolic monitoring
Trauma and critically ill patients often exhibit profound alterations in biochemical markers due to systemic inflammation and metabolic stress. Visceral proteins such as albumin, prealbumin, and transferrin are traditionally used to assess nutritional status. However, during acute inflammatory phases, these markers are significantly influenced by systemic inflammation and may not reliably reflect malnutrition [4, 11]. C‑reactive protein (CRP) and procalcitonin (PCT) provide insights into inflammation, helping differentiate nutritional deficits from inflammatory changes in visceral protein levels [8, 23].
Electrolyte imbalances, including hypophosphatemia, hypokalemia, and hypomagnesemia, are common in trauma patients with significant fluid shifts or blood loss as well as in critically ill patients initiating refeeding after prolonged fasting. These imbalances are hallmark features of refeeding syndrome and require meticulous monitoring during initiation of nutritional support to prevent life-threatening complications [7, 21]. Glycemic control is another cornerstone of metabolic monitoring. Hyperglycemia, often observed in patients receiving TPN, is associated with an increased infection risk, impaired wound healing, and higher mortality rates [18].
Specialized nutritional strategiesImmunonutrition
Trauma patients, especially those with severe injuries such as major fractures, burns, or polytrauma, often exhibit a heightened inflammatory response that makes them particularly suitable for immunonutrition strategies. Formulations enriched with omega‑3 fatty acids, arginine, and glutamine have demonstrated benefits in modulating this hyperinflammation, reducing oxidative stress, and supporting immune responses. These supplements are critical for promoting wound healing and improving clinical outcomes in trauma patients [1, 23].
Antioxidants and micronutrients
Supplementation with antioxidants such as vitamin C, selenium, and zinc is increasingly recognized for its role in reducing oxidative stress and supporting immune function, particularly in critically ill patients with prolonged illness or extensive tissue damage ([1, 11, 20]; Table 2).
Table 2 Micronutrient recommendationsHigh-protein diets
Tailored formulations with increased protein content are essential for counteracting catabolism, promoting wound healing, and maintaining lean body mass. Protein intake recommendations range from 1.5–2.5 g/kg/day, depending on the severity of the injury or illness [2, 20, 22].
Emerging technologies and advanced monitoring tools
Advanced technologies are transforming nutritional monitoring in trauma and critically ill patients. Bioimpedance analysis (BIA) is a noninvasive method gaining traction for assessing body composition and tracking changes in lean mass and fluid status over time [18]. Exhaled CO2 analysis shows promise as an alternative to indirect calorimetry for estimating energy expenditure, particularly in unstable patients for whom traditional methods may not be feasible [17].
Multidisciplinary approach
A coordinated multidisciplinary approach is essential for successful implementation and monitoring of nutritional support. Collaboration among intensivists, general surgeons, trauma surgeons, dietitians, nurses, and pharmacists ensures that nutritional strategies are dynamically adjusted to the patient’s evolving clinical condition [18]. Regular interdisciplinary discussions address challenges such as feeding intolerance, refeeding complications, and the need for specialized formulations [21].
The review identified several critical aspects of nutritional support in trauma and critically ill patients, including energy estimation, protein requirements, timing, delivery methods, and monitoring strategies. These findings are synthesized and summarized in Table 3, which provides a concise overview of the key nutritional recommendations tailored to these populations.
Table 3 Nutritional recommendations for trauma and critically ill patients




Comments (0)