The management of patients with giant scrotal hernias and their medical treatment is usually challenging, not only from a surgical/technical point of view, but also due to the frequently present multiple comorbidities and undiagnosed conditions in this oftentimes medically undertreated patient cohort.
Several open and laparoscopic repair options for hernia repair exist for this specific condition, which usually requires a multidisciplinary, team-based approach throughout its treatment. The early involvement of a dedicated hernia surgeon’s expertise, however, is essential [1,2,3].
In order to avoid emergency procedures without any time for in-depth diagnosis and sufficient treatment of comorbidities in these challenging cases, it is essential to establish a tailored plan for this relatively small subset of hernia patients.
Prehabilitation of patients, optimization of risk factors, and preconditioning of the future surgical fields, if necessary, in as timely a manner as possible, includes the evaluation and correction of malnutrition and iron deficiency, optimization of antidiabetic treatment, reduction of excessive bodyweight, management of cardiovascular and pulmonary diseases, timely or permanent smoking cessation, bacteriologic or infectiologic screening, and meticulous planning of the actual surgical procedure.
Aside from all other factors influencing postoperative adverse events and outcomes, an additional risk for patients with large hernias associated with loss of domain is reflected by abdominal compartment syndrome [11].
To reduce the likeliness of its manifestation, either the volume of the hernia sac’s content needs to be reduced, or the volume of the abdominal cavity needs to be increased [1]. The first can generally be achieved by resection of viscus or omentum, the latter by use of progressive pneumoperitoneum (PPP) [5,6,7], surgical component separation (CS), or staged closure of the abdominal cavity [5]. All of these options are resource and time consuming and, as invasive measures, they bear the risk of additional morbidity and adverse outcomes for the patients.
Another option—to date hardly implemented in the management of large scrotal hernias—is preoperative injection of the abdominal wall’s lateral muscles with botulinum toxin A. Compared to the described alternatives, it is a clearly less-invasive and time-consuming alternative. Over time, it leads to a predominant increase of the abdominal cavity’s volume, whereas PPP naturally also temprarily increases the inguinal hernia sac’s volume [12].
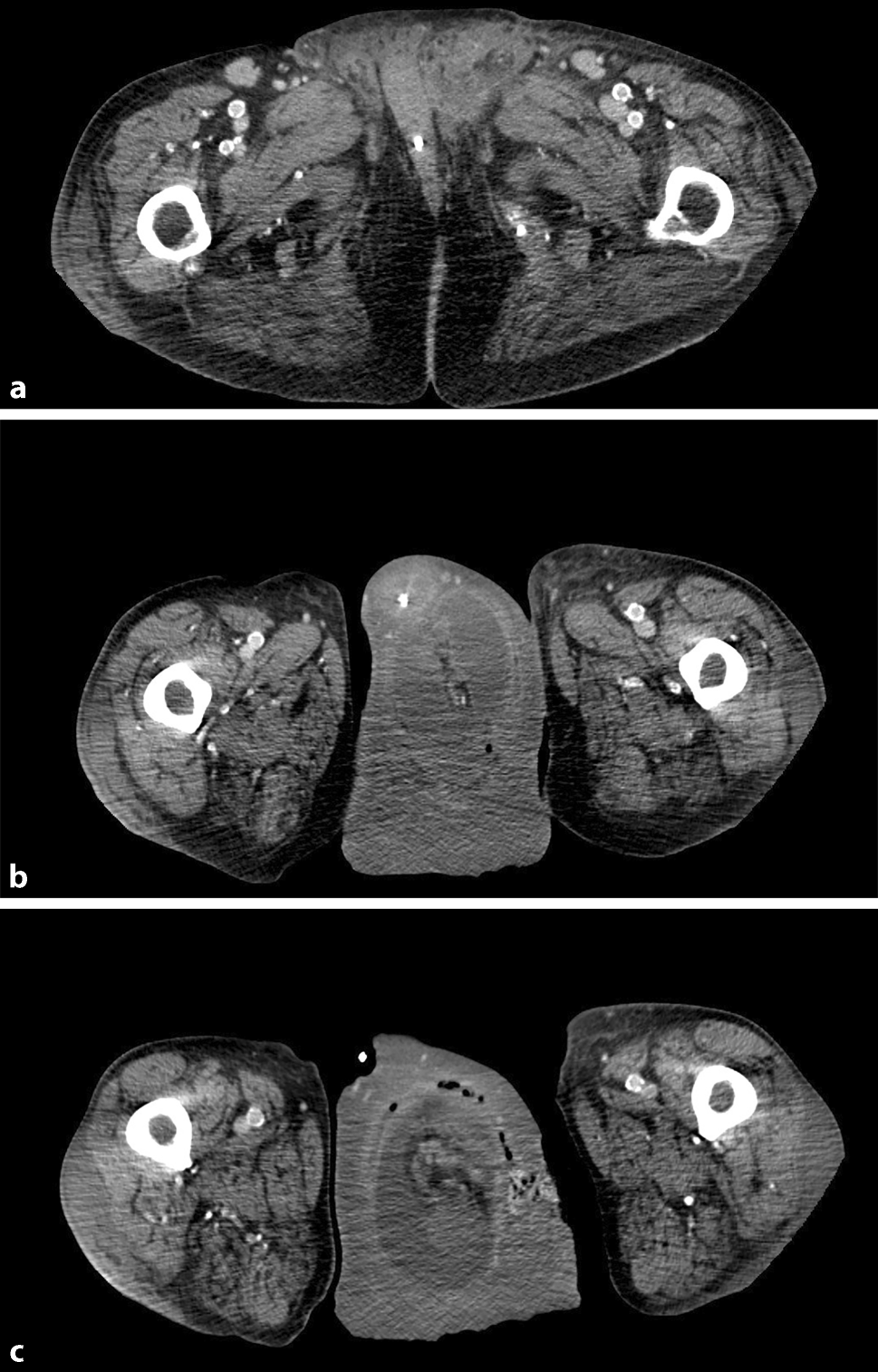
A generally accepted method for the measurement of hernia sac and intra-abdominal cavity volumes for large inguinoscrotal hernias has not been presented to the best of our knowledge. Both Tanaka et al. [7] and Sabbagh et al. [13] focused on incisional hernias in their work and provided techniques for measurements of the respective volumes. For the preoperative work-up of this case, Tanaka’s method and the described modifications were chosen. Relevant studies focusing on the peculiarities of volume measurements in inguinoscrotal hernias are still lacking, but volume calculations appear mandatory for these patients and should be considered an inherent part the preoperative work-up.
The hernia classification EHS pL3 is documented in the original theatre report. Since scrotal hernias generally tend to be EHS L3, further classification is warranted in these cases: Trakarnsagna et al. [14] suggest a classification of three grades with the hernia sac reaching to the mid-inner thigh (grade 1), to the suprapatellar lines (grade 2), or to the superior border of the patellar bone (grade 3) in their publication. According to this proposed recommendation, the case we present would be described as grade 3. In view of the consensus paper published by 25 surgeons of the HerniaSurge group in 2023 [15], the hernia described in this manuscript could be graded as S3 (IR) despite a very low level of evidence and weak strength of recommendation.
The described case shows that botulinum toxin A can be a valuable component of the hernia surgeon’s toolbox—not only in ventral, but also in large scrotal hernias with loss of domain. In view of the low number of published cases, it must be assumed that only a few surgeons currently use the technique for the management of these scrotal hernias. The underlying reason might be either the relatively low number of truly giant inguinal hernias in countries with readily available medical botulinum toxin A or the fact that the correlation between a treatment of the abdominal wall’s lateral muscles and the actual scheduled procedure well away from them in the groin is not initially obvious and, therefore, frequently overlooked.
Thorough preoperative planning, careful patient prehabilitation, and preconditioning of the extended surgical field can help to avoid an intraoperative impossibility of hernia content reduction into the abdomen, the need for additional surgical emergency measures in order to make reduction possible, or even forced reduction, which is associated with acutely elevated intra-abdominal pressure and an increased risk of the manifestation of ACS.
Open anterior mesh-augmented repair was considered the default procedure for scrotal hernias in most cases and for the majority of surgeons [15] in 2023. Implant size should reflect the size of the hernia defect and must naturally be adapted to the patient’s anatomy. In hindsight, further mesh fixation in addition to the medially placed nonabsorbable suture could have been considered. The implant chosen for the procedure described proved sufficient for the hernia repair until the end of the patient’s life.
Excessive scrotal tissue may not require resection due to its ability to shrink. However, scrotal hematoma is not uncommon and secondary skin resection may be found necessary [15].
For the presented case, a definitive repair in one operation was aimed for in view of the patient’s multimorbid condition. In hindsight, local complications could not be avoided and might have warranted a less-invasive approach despite the large amount of residual scrotal skin after intraoperative reduction of the hernia.
Zuvela et al. [16] doubt the efficacy of Lichtenstein’s repair for very large inguinoscrotal hernias. The authors present a case series with a median hernia defect size of 10 cm and including absurdly gigantic hernia sacs. For these very large hernias, favorable results could be achieved with preperitoneal repair techniques with or without very extensive additional surgical measures. While it appears next to impossible to achieve sufficient coverage of these giant defects with Lichtenstein’s technique, the procedure has proven suitable for smaller defects like the one presented in the current case.
The chosen treatment for this patient proved sufficient for the rest of his life and outlines the multiple difficulties potentially encountered in the management of large scrotal hernias. Due to the ongoing lack of robust available evidence with regard to best practice for the management of the affected patients, additional research remains important to achieve the best possible results. A carefully tailored approach remains a cornerstone of the affected patients’ successful treatment. Recent publications appear to support this fact.
Even though the small number of published cases makes further evaluation of the technique for giant scrotal hernias necessary, the presented case confirms the facilitated repair after BTA infiltration.
A multi-year postoperative follow-up according to the Herniamed register’s standards would clearly have been desirable. However, the patient’s demise for causes unrelated to the surgical procedure once again shows the usually associated extensive comorbidity profile and highlights the significance of meticulous preoperative planning of this not only surgically demanding cohort [17].




Comments (0)