This multicenter, prospective, observational trial enrolled adult patients (≥ 18 years) admitted to 10 ICUs in Henan Province, China, between August 2021 and August 2023. The study was approved by the institutional review board or independent ethics committee at each site and adhered to the Declaration of Helsinki, the International Conference on Harmonisation Good Clinical Practice, and relevant regulations in China. Written informed consent to participate was obtained from each patient or their legally authorized representative before study participation. Data were collected and recorded by specified physician in each site. An independent monitoring board periodically reviewed the trial outcomes and safety. Earlier data from the current study had been analyzed previously [8], while the present analysis involved the trail’s full dataset, with 67 duplicated patients involved in both.
Patients (≥ 18 years) hospitalized with severe infections caused by CROs and confirmed through microbiological culture and antimicrobial susceptibility testing of clinically relevant specimens were enrolled. Exclusion criteria included pregnancy or breastfeeding, documented hypersensitivity to polymyxins, recent polymyxin therapy (within 7 days before enrolment), or anticipated survival < 4 days. Patients were followed for clinical outcomes for up to 28 days or until discharge, whichever occurred first.
Patients received colistin sulfate (Shanghai SPH New Asia Pharmaceutical Co. Ltd., Shanghai, China) with loading doses of 1.0 or 1.5 million international units (IU), maintenance doses of 1.0 or 1.5 million IU daily, divided into two or three doses, via intravenous infusion over 1 h. Every 0.5 million IU colistin sulfate was reconstituted in 100 mL normal saline to obtain a 5000 IU/mL solution. Nebulized colistin sulfate was initiated at the discretion of the treating physician based on the patient’s condition for patients with pulmonary infection, at a dosage of 0.25 or 0.5 million IU every 12 or 24 h over 30 min via the vibrating mesh nebulizer. Each 0.5 million IU of colistin sulfate was reconstituted with 10 mL of normal saline to obtain a 50,000 IU/mL inhaled solution. No dose adjustments were required for patients on continuous renal replacement therapy (CRRT) or extracorporeal membrane oxygenation (ECMO). Combination with carbapenems, tigecycline, ceftazidime-avibactam, or other guideline-recommended antibiotics was permitted as per the treating physician’s discretion. The duration and final dosage of treatment were physician determined.
Carbapenem resistance was defined as resistance to imipenem and meropenem in antimicrobial susceptibility testing. Bacterial susceptibility to antimicrobials in susceptibility testing are included in the Supplementary Information. CRO infection was assayed and confirmed in all patients at screening. Clinical specimens, including bronchoalveolar lavage fluid (BALF), sputum, blood, urine, wound secretions, cerebrospinal fluid, etc., obtained within 48 h before the first study treatment dose, were processed locally for culture and susceptibility testing, adhering to the Clinical and Laboratory Standards Institute (CLSI) guidelines (M100) [13]. Isolates with a minimum inhibitory concentration (MIC) of ≤ 2 mg/L using broth microdilution methods were considered susceptible to colistin sulfate according to the European Committee for Antimicrobial Susceptibility Testing [14]. A semiquantitative analysis was employed for sputum specimens with a threshold of ≥ 105 colony-forming units (CFU)/mL, while a quantitative analysis was used for BALF specimens with a threshold of > 104 CFU/mL. Clinical diagnosis of sepsis or septic shock followed the Surviving Sepsis Campaign guideline [15]. Blood samples were also collected to explore colistin sulfate pharmacokinetics, with results to be presented in a separate publication.
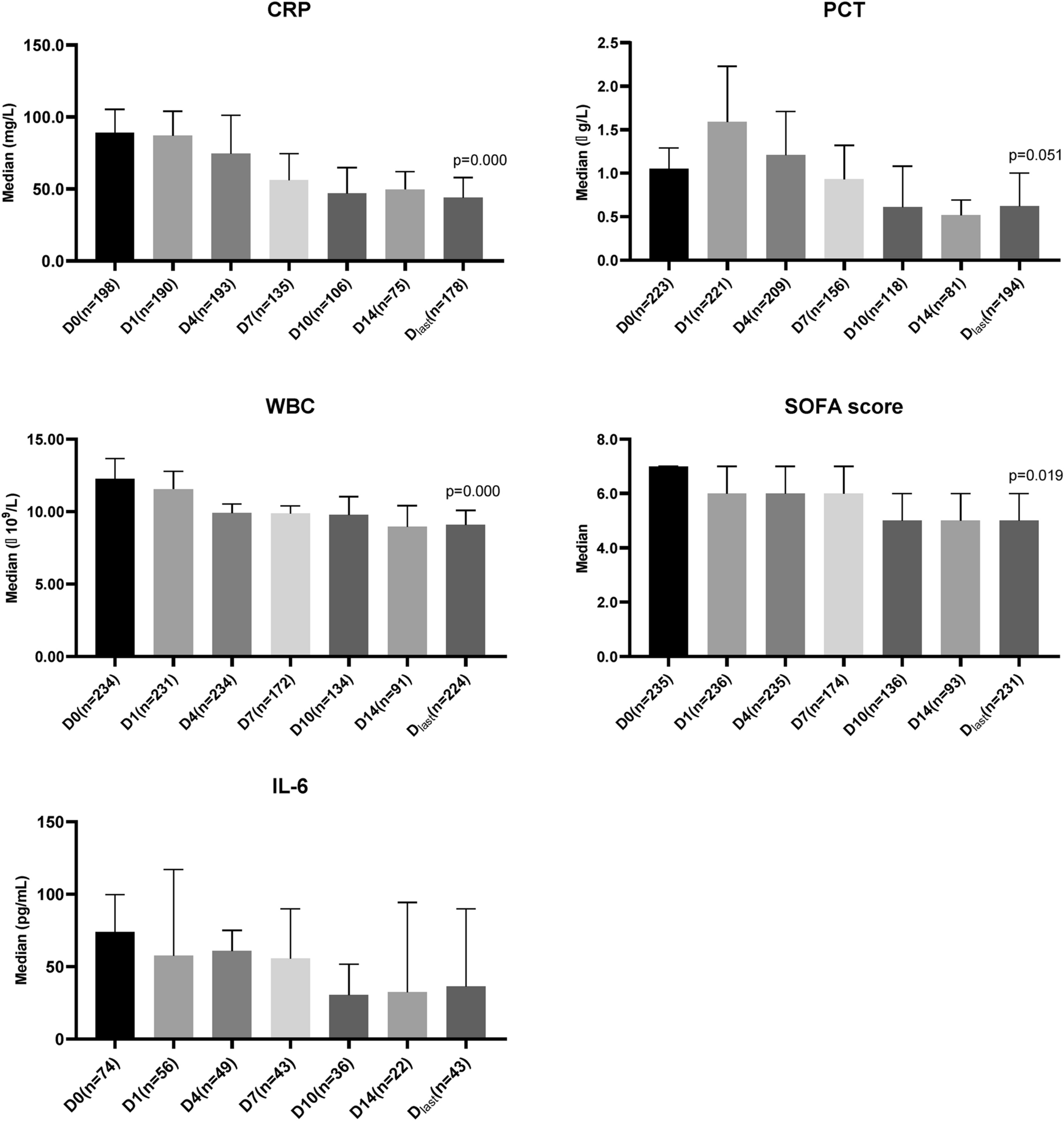
The primary efficacy outcomes focused on the clinical and microbiological response following treatment. Clinical response was defined as the resolution or relief of signs and symptoms of CRO infection, alongside improvements in laboratory and/or imaging findings at the end of colistin sulfate treatment. The positive outcome is based on fever defervescence, reductions in sputum volume/suctioning requirements; vasoactive drug dose; decrease in Sequential Organ Failure Assessment (SOFA) score and interleukin-6 (IL-6); improvements in arterial blood gas and organ function; normalization of white blood cell (WBC), C-reactive protein (CRP), and procalcitonin (PCT); and decrease or resolution of findings on chest X-ray. Conversely, clinical failure was defined as the persistence or worsening of infection signs and symptoms, without observable improvement in laboratory and/or imaging outcomes after discontinuation of colistin sulfate. Clinical responses were determined by consensus of two physicians who were blinded to the microbiological results. Microbiological eradication was defined as the absence of pathogenic bacteria in the cultures from the primary infection source at the end of colistin sulfate treatment. Presumed eradication was defined as absence of microbiological results in clinically cured patients due to lack of culturable specimens (e.g., sputum, skin pus, or secretions) or for whom obtaining culturable specimens was too invasive for the recovered patient. Microbiological eradication and presumed eradication were combined as microbiological response. The secondary efficacy outcomes included the changes in other indicators (i.e., SOFA score, levels of WBC, CRP, PCT, and IL-6), and 28-day all-cause mortality. The 28-day all-cause mortality was defined as death from any cause within 28 days from start of colistin sulfate treatment, regardless of whether the death occurred in the ICU, after transfer to a regular ward, or following hospital discharge. Safety assessments focused on nephrotoxicity and neurotoxicity, with special emphasis on nephrotoxicity due to the critical condition of patients in ICUs. Drug-related nephrotoxicity was evaluated according to Kidney Disease Improving Global Outcomes (KDIGO) criteria, identifying acute kidney injury (AKI) via serum creatinine (Scr) levels. The baseline Scr level was defined as the last test result before the first dose of colistin sulfate. AKI cases in patients with preexisting renal impairment or those undergoing CRRT were excluded from the drug-related nephrotoxicity analysis to differentiate between disease progression and drug-induced effects. AKI status in patients with CRRT was diagnosed based on Scr levels before CRRT initiation, according to the KDIGO criteria. Clinical judgement guides CRRT initiation based on indications including hemodynamic instability, fluid overload, severe electrolyte and/or acid–base imbalance, and sepsis requiring the removal of inflammatory mediators. Combination therapy was defined as any use of an antibiotic in addition to colistin sulfate from the commencement of colistin sulfate treatment.
The sample size was calculated based on clinical response in critically ill patients, assuming a response rate of 70% (literature range: 70–90% [9, 12]). The calculated sample size (N) was 221 by using a permissible error (δ) of 10%, a two-tailed significant level (α) of 0.05, a power (1 − β) of 0.9, as determined by the following formula:
$$N = p(1 - p)\frac + \mu_ )}} }}$$
, where μ is the quantile of the standard normal distribution. Accounting for a 10% drop-out rate, 246 patients were required to be enrolled.
The final analysis included eligible patients receiving ≥ 4 days of colistin sulfate therapy with complete data. Missing variables were imputed using the mean of the cohort or subgroup if ≥ 90% of values were available; otherwise, no imputation was performed. Subgroup analyses assessed age, pathogen type, infection site, life support use, and treatment duration that may affect clinical outcomes or are clinically important, based on similar studies [16, 17].
The data are reported as percentages (%), mean ± standard deviation or median with interquartile range (IQR) as appropriate. Categorical variables were compared using the chi-square (χ2) test or Fisher’s exact test, while continuous variables were compared using either the t-test or the Wilcoxon rank-sum test. Bonferroni correction of p-values was applied for multiple comparison analysis. Multivariate logistic regression analysis (method: Forward, Wald, α = 0.05) was used to identify risk factors for clinical failure or mortality. Variables with a p-value of < 0.1 were entered into a multivariate logistic regression analysis. In addition, factors of clinical importance were forced entered the model. The Hosmer‒Lemeshow test was used to evaluate the goodness of fit for the model. The collinearity among variables was examined using multiple linear regression. The correlation between variables were assessed using the Pearson correlation coefficients. Statistically significant correlations with coefficients ≥ 0.3 were considered clinically meaningful. The receiver operating characteristic (ROC) curve was used to evaluate the predictive thresholds of each predictor. Propensity score matching (PSM) was used to adjust for confounders between the intravenous plus inhaled and intravenous colistin sulfate groups for patients with infection solely at the pulmonary site. Variables related to clinical response and mortality with a p-value < 0.1 in the univariate analysis (Supplementary Tables 4 and 7) were included in the propensity score. The two groups were matched at a ratio of 1:1 with a caliper width of 0.1. All analyses were performed using SPSS software, version 26.0. A two-tailed p-value < 0.05 was considered significant.




Comments (0)