
Remember me




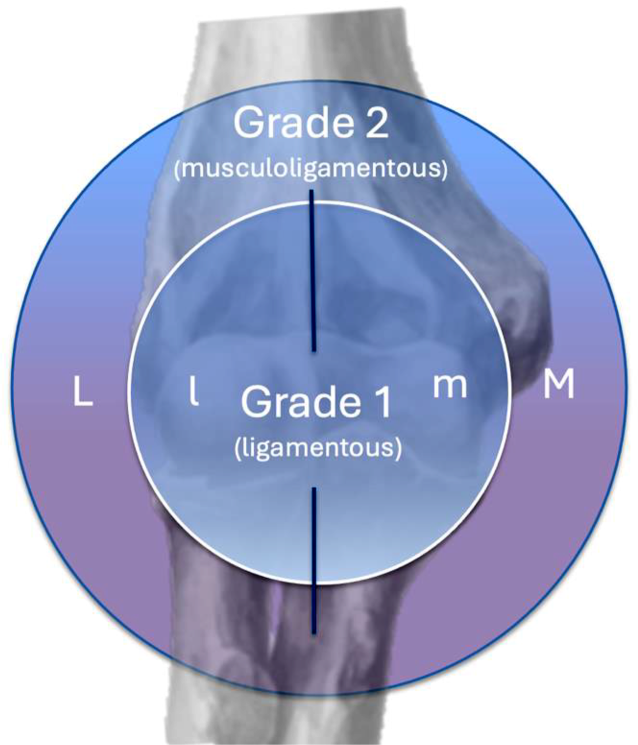



Clinical classifications should not only serve an academic purpose but should also incorporate a clear treatment strategy. The Munich Elbow Soft Tissue (MEST) classification is an MRI-based classification system for acute simple elbow dislocations that distinguishes two grades of severity—(1) isolated ligamentous injuries and (2) musculoligamentous injuries (complete disruption of ligaments and muscles)—with three subtypes based on the main pathology in relation to its location (lateral, medial, or bilateral; Fig. 1). Furthermore, treatment recommendations are derived from this grading system.
The following classification builds on a retrospective case review from January 2011 to July 2023 based on MRI scans of 134 patients who had an acute simple elbow dislocation (< 30 days) without any bony injuries. Figure 1 shows the individual subgroups of the classification system.
Fig. 1
The Munich Elbow Soft Tissue (MEST) classification circle. Grade 1 injuries represent isolated ligamentous tears (lowercase letters), while grade 2 injury patterns involve complete musculoligamentous tears extending into the subcutaneous soft tissue (uppercase letters). Medial (M, m) and lateral (L, l) indicate the main pathology
Grade 1The main MRI finding in this group is a complete separation of the ligamentous stabilizers with intact dynamic stabilizers (muscle–tendon attachments) or a partial lesion of these on MRI (not extending more than 50% of the tendon insertion). Depending on the location of the injury, a distinction into the three subtypes is made. Thus, this group is defined as follows: ligament rupture with preserved muscle integrity.
Grade 1l: lateralOn coronal and axial MRI sections, a disruption of the lateral ulnar collateral ligament (LUCL) can be identified. Depending on the severity, a partial rupture of the extensors can be observed in terms of fluid (bleeding) within the muscle fibers. However, the continuity of the muscle–tendon unit to the lateral epicondyle should be maintained (Fig. 2, [19]).
Fig. 2
Coronal view (a) with complete disruption of the humeral lateral ulnar collateral ligament insertion (arrow). Axial view (b) with strained extensor origin (asterisk)
Immobilization is recommended for a maximum of 3–5 days in an upper arm splint followed by soft tissue consolidation through lymph drainage and exercising of the hand and shoulder joint. This is followed by transfer to an elbow brace for 4 weeks: weeks 1–2, extension/flexion limited to 0°-20°-90° in pronation (no active pronation/supination) for ligament preservation; weeks 3–4, 0°-10°-110° (free pronation/supination), with passive and active-assisted motion in overhead position [20,21,22,23,24,25].
Grade 1m: medialOn coronal and axial MRI sections, a complete disruption of the MCL course on the humeral or ulnar side can be observed. Depending on the severity, a partial tear of the flexors can be observed in terms of fluid (bleeding) within the muscle fibers. However, the continuity of the muscle–tendon unit to the medial epicondyle should be maintained (Fig. 3; [26]).
Fig. 3
Coronal view (a) with complete disruption of the humeral medial collateral ligament insertion (arrow). Axial view (b) with strained flexor origin (asterisk)
Immobilization is recommended for a maximum of 3–5 days in an upper arm splint followed by soft tissue consolidation through lymph drainage and exercising of the hand and shoulder joint. This is followed by transfer to an elbow brace for 4 weeks: weeks 1–2, extension/flexion limited to 0°-20°-90° in supination (no active pronation/supination) for ligament preservation; weeks 3–4, 0°-10°-110° (free pronation/supination), with passive and active-assisted motion in overhead position [25, 27, 28].
Grade 1l-1m: bilateralCoronal and axial MRI sections show a complete disruption of the LUCL and MCL course mainly on the humeral side. Depending on the severity, intratendinous partial tears of the extensors and flexors can be observed in terms of fluid (bleeding) within the muscle fibers. However, the continuity of the muscle–tendon unit to the lateral and medial epicondyle should be maintained (Fig. 4).
Fig. 4
Coronal view (a) with complete disruption of the humeral medial collateral ligament and lateral ulnar collateral ligament insertions (arrows). Axial view (b) with strained flexor and extensor origins (asterisk)
Immobilization is recommended for a maximum of 3–5 days in an upper arm splint followed by soft tissue consolidation through lymph drainage and exercising of the hand and shoulder joint. This is followed by transfer to an elbow brace for 4 weeks: weeks 1–2, extension/flexion limited to 0°-20°-90° in neutral position (no pronation/supination) for ligament preservation; weeks 3–4, 0°-10°-110° (free pronation/supination), with passive and active-assisted motion in overhead position [20,21,22,23, 27, 29].
Grade 2In this group, the main feature is a complete separation of the ligamentous and the muscular elbow stabilizers with a detached capsule–ligament–muscle–tendon unit seen on MRI sections. Depending on the location of the injury, a distinction into the three subtypes is made. Thus, this group is characterized as ligament rupture combined with muscular instability.
Grade 2L: lateralOn coronal and axial MRI sections, a disruption of the LUCL can be identified. Furthermore, a complete separation of the extensor muscle insertions can be identified, with fluid between the lateral epicondyle and the tendon stump or the tendon stump and muscles (Fig. 5).
Fig. 5
Coronal view (a) with complete disruption of both the humeral lateral ulnar collateral ligament (arrow) and the extensor origin (asterisk). Axial view (b) with complete rupture of the extensor and lateral ulnar collateral ligament origin (asterisk, arrow)
The treatment recommendation for active patients, especially those with high functional demands and/or participating in (upper extremity) sports, involves surgical refixation (LUCL and extensor muscle insertions) via a lateral approach in the acute phase (< 3 weeks). In our patient cohort, despite having similar clinical outcomes, we observed a faster return to sports in the surgically treated group compared to the group with conservative management [12]. Furthermore, 10% of the conservative group complained of severe subjective instability at the final evaluation [12]. While a faster return to sports was observed in young and active patients following surgery, older patients with low functional demands did not benefit in the same way. Since the current literature still suggests similar outcomes following conservative management, these patients are referred for short-term immobilization followed by early mobilization (see grade 1 lateral injuries; [6, 7]).
Grade 2M: medialOn coronal and axial MRI sections, a complete disruption of the MCL course on the humeral or ulnar side and of the flexors can be observed in terms of fluid between the medial epicondyle and the tendon stump or between the tendon stump and muscles (Fig. 6).
Fig. 6
Coronal view (a) with complete disruption of both the humeral medial collateral ligament (arrow) and the flexor origin (asterisk). Axial view (b) with complete rupture of the flexor origin (asterisk)
For active patients, especially those with high functional demands and/or participating in (upper extremity) sports, a surgical refixation (MCL and flexor muscle insertions) via a medial approach in the acute phase (< 3 weeks) can be recommended [12, 30]. For older patients, individuals with low functional demands, and those with contraindications to surgical management, short-term immobilization is recommended followed by early mobilization, as detailed in the treatment of grade 1 medial injuries.
Grade 2L-2M: bilateralOn coronal and axial MRI sections, a complete disruption of the LUCL and MCL course, mainly on the humeral side, as well as a complete tear of the extensors and flexors is seen (Fig. 7).
Fig. 7
Coronal view (a) with complete disruption of all static and dynamic collateral stabilizers including the humeral medial collateral ligament and lateral ulnar collateral ligament (arrows) and the flexor and extensor origins (asterisk). Axial view (b) with complete rupture of bilateral flexor and extensor origins (asterisk)
The treatment recommendation for active patients, especially those with high functional demands and/or participating in (upper extremity) sports, comprises surgical refixation (LUCL + extensors and MCL + flexors) via a bilateral approach in the acute phase (< 3 weeks; [7, 12, 30]). For older patients, individuals with low functional demands, and those with contraindications to surgical management, short-term immobilization is recommended followed by early mobilization, as detailed in the treatment of grade 1 bilateral injuries.
Comments (0)