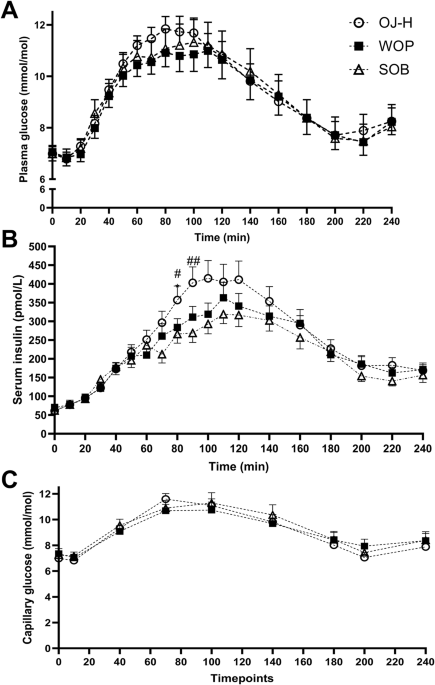
Evidence-based, realistic dietary advice is needed for people with T2DM to manage and improve their condition and overall cardiometabolic health. Increasing fruit and vegetables is one aspect of this, as it is for the general healthy population, but the role of 100% fruit juice (i.e., no added sugars, as described in the Reference Guidelines of the European Fruit Juice Association’s Code of Practice) requires further clarification, especially for populations with diabetes. Contrary to expectations, the current study found no significant differences in acute glucose or insulin responses when either whole orange pieces, orange juice or a sugar-sweetened control beverage identical in total sugar content were consumed with a standard meal rich in carbohydrates. One reason for this could be that the carbohydrate load of the three test options (~22 g) contributed to a lesser extent to the observed glycaemic responses when compared with the carbohydrate load of the breakfast meal (~80 g). Intriguingly, it appears that certain nutritional aspects of whole orange pieces (containing hesperidin and fibre) and 100% orange juice (containing hesperidin) were insufficient to influence the overall glycaemic response when consumed with a carbohydrate-rich meal. In this context, the inherently high variability of the composition of fruit pieces as compared to the homogeneous composition of the orange juices sourced from a single batch should be highlighted (Table 2).
As the potential health benefits of dietary polyphenols is a growing field of interest in nutritional science, previous studies in populations without T2DM have found that experimental hesperidin, which remains unmodified until it reaches the colon, decreases postprandial glycaemia via GLUT-2 inhibition [10]. GLUT-2 transporters at the basolateral membrane of the enterocytes (i.e., small intestine) make passive diffusion of glucose/fructose/galactose possible into the bloodstream. However, in insulin-resistant individuals with obesity, GLUT-2 is known to accumulate in the apical membrane, allowing glucose to passively diffuse into the bloodstream [15]. Although the orange juice and whole orange pieces in the current study were consumed in an acute setting, our findings appear to be in line with previous study results which showed that individuals with obesity and/or a reduced insulin sensitivity, as is typically the case in T2DM, hamper any hesperidin-related glucose lowering effects [16]. Moreover, a 12-week intervention with daily 100% orange juice versus a sugar-matched orange-coloured drink in overweight and insulin-resistant men reported no alterations in carbohydrate or lipid metabolism [17]. Since beta-cell functional capacity (often expressed by the proxy HOMA-β [14]) is a known parameter (at least partly) determining acute glycaemic control, being related to metabolic clearance rates of endogenous insulin or the acute induction of insulin resistance [18], we observed a heterogenous range (i.e., HOMA-β 28–132%) among the individuals included. Therefore, it is tempting to speculate that this variation in beta-cell function might have blunted the current studied glycaemic responses. Unfortunately, the current study lacked statistical power to perform secondary analyses based on BMI or HOMA- β.
Interestingly, as no differences in glycaemic control between experimental conditions were found in our acute study, the current data may indicate the importance of colonic modification (as reviewed by Mas-Capdevila et al. [19]). Indeed, the cardiometabolic health benefits of citrus flavonoids, like hesperidin, on postprandial carbohydrate metabolism may not solely rely on small intestinal function. Factors like inhibitory effects on intestinal α-glucosidase, gut microbiota composition, substrate utilisation or mitochondrial function may impact these effects in metabolically compromised individuals [20,21,22].
Although our study did not investigate the chronic effects of fruit juice consumption, we note that the recommendations of the European Association for the Study of Diabetes which state that “the evidence for benefits for 100% fruit juice appears restricted to levels of intake obtainable from a single piece of fruit (≤150 ml)”. In accordance with this statement, our results suggest that a single serving of orange pieces or 100% orange juice with a meal does not have a detrimental effect on glycaemic control in people with T2DM. Nevertheless, fruit juices are certainly sugar-containing beverages and, according to numerous dietary recommendations [4], they should only be consumed occasionally. Unlike fruit juices, sugar-sweetened beverages do not contain similar vitamins, minerals and natural bioactive compounds as fruits. Therefore, sugar-sweetened beverages remain inadvisable for people with T2DM, despite the findings of this study.
The main limitations of the current intervention include the small sample size, limiting the detection of small differences in (potential metabolically important) glycaemic outcomes, and the partial blinding of the participants. However, experimental visits were randomised so it is unlikely that a single postprandial intervention would change the response to the next experimental visit (minimal break of 5 days between experimental visits). Strengths of the intervention include the measurement of glucose using both venous and capillary methods, the standardisation of the orange juice and the measurement of hesperidin in both the orange juice and all 16 individual batches of the served whole orange pieces. Future studies should examine the long-term impact of eating fruit versus drinking fruit juice on glycaemic control and insulin sensitivity in people with T2DM, considering more robust or sensitive markers other than AUC, such as glycated haemoglobin.
In conclusion, our results indicated no differences in acute glycaemic control in individuals with well-controlled T2DM following a single serving of orange juice, whole orange pieces or a sugar-sweetened beverage with a standard high-carbohydrate meal. In addition, given the similarity of outcomes for the two orange conditions (containing hesperidin) and the sugar-sweetened beverage control (no hesperidin), a single dose of hesperidin had no acute impact on glycaemic control.

Comments (0)