
Remember me


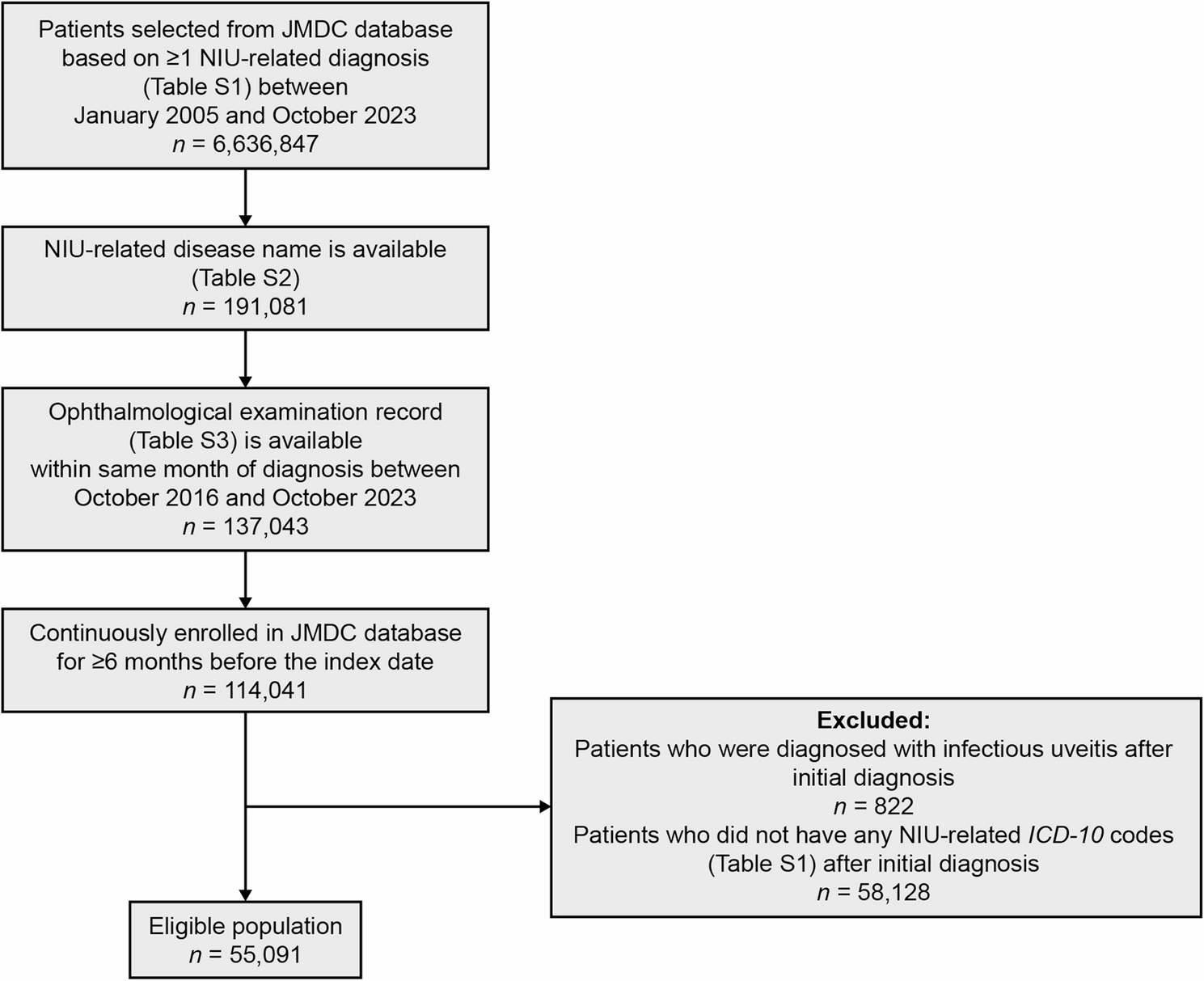


A total of 55,091 patients with an NIU-related diagnosis met the eligibility criteria (Fig. 1). In 2023 (N = 13,278,370), the estimated (95% CI) prevalence of NIU in the JMDC database was 313.2 (310.2–316.3) per 100,000 persons, and estimated (95% CI) prevalence of UME was 20.9 (20.1–21.7) per 100,000 persons. For the overall cohort, the mean (± standard deviation [SD]) age was 44.9 (16.9) years, with nearly half of all patients aged 40–59 years (Table 1), and half (50.9%) were male. Most patients were given at least one treatment for NIU (87.7%, 48,318/55,091), with 68.7% of the overall cohort given treatment for mild NIU with corticosteroid eye drops only (37,869/55,091), and a further 19.0% (10,449/55,091) were given other treatments for moderate-to-severe NIU throughout the study period (Table 1; Fig. 2). The mean (± SD) time from the index date to the end of the observation period was 1,018.3 (678.3) days (or a mean 2.8 years) for the overall cohort, 999.5 (674.2) days (or a mean 2.7 years) for patients with mild NIU, and 1,168.5 (688.9) days (or a mean 3.2 years) for patients with moderate-to-severe NIU (Table 1).
Fig. 1
Patient attrition of eligible patients with NIU from the JMDC database. The index date, also referred to as the first encounter, is the date of the initial ophthalmological examination record (between October 1, 2016 and October 31, 2023) confirming NIU diagnosis. ICD, International Classification of Diseases, Tenth Revision; JMDC, Japan Medical Data Center; NIU, non-infectious uveitis
Table 1 Patient demographics and clinical characteristics (at index datea) of patients with NIUFig. 2
Proportion of all eligible patients with NIU in the JMDC database receiving corticosteroid eye drops (for mild NIU), other treatments (for moderate-to-severe NIU), or no treatment for NIU. JMDC, Japan Medical Data Center; NIU, non-infectious uveitis
Of patients with NIU diagnoses most commonly reported in Japan [29], 3.2% were confirmed to have sarcoidosis, 2.0% Behçet’s disease, and 1.2% VKH disease. Approximately 95% of patients had “other” NIU diagnoses, including scleritis/episcleritis, unclassified uveitis, iritis, and iridocyclitis. For uveitis-related ocular diseases, < 1% of patients had UME and < 2% had ERM in the 6 months before the study period. Overall, 8.7% of patients (4,767/55,091) were diagnosed with a systemic disorder associated with NIU (ICD-10 codes listed in Table S7) during the 6 months before NIU diagnosis, most commonly diabetes and spondylosis. However, for moderate-to-severe NIU, a larger proportion of patients were diagnosed with a systemic disorder (11.7%) than patients with mild NIU (6.3%). In addition, 18.4% of patients with moderate-to-severe NIU had a history of treatment for systemic disorders related to NIU (defined in Table S7), versus 2.0% of patients with mild NIU.
Treatment selectionAmong patients with moderate-to-severe NIU, the most common initial treatments (except for corticosteroid eye drops) were oral corticosteroids (63.1%), followed by local corticosteroid injections (posterior sub-Tenon’s [12.6%] and subconjunctival [8.6%]), intravenous injections (6.8%), oral immunosuppressants (6.4%), and colchicine (4.0%) (Fig. 3, Tables S8 and S9). Patients with UME or ERM in the 6 months before NIU diagnosis were more likely to receive initial treatment with posterior sub-Tenon’s corticosteroid injections (UME: 49.4%, 76/154; ERM: 36.5%, 73/200) than all patients with moderate-to-severe NIU (12.6%, 1,320/10,449). By the end of the study, the most common treatments for patients with moderate-to-severe NIU (except for corticosteroid eye drops) were generally consistent with initial treatments used: oral corticosteroids (71.5%), local corticosteroid injections (posterior sub-Tenon’s [15.7%] and subconjunctival [10.0%]), intravenous injections (10.7%), oral immunosuppressants (10.6%), and colchicine (5.3%) (Fig. 3, Tables S10 and S11).
Fig. 3
Proportion of patients with moderate-to-severe NIU receiving treatments other than corticosteroid eye drops. Treatments taken at the first encounter (index date) and all treatments taken by the last encounter are both presented (note that patients may have received multiple treatments). Infliximab and adalimumab are TNF-α inhibitors. ADA, adalimumab; Col, colchicine; IFX, infliximab; inh, inhibitor; inj, injection; IS, immunosuppressant; IV, intravenous; IVT, intravitreal; JAK, Janus kinase; NIU, non-infectious uveitis; PDE4, phosphodiesterase-4; SCJ, subconjunctival; ST, sub-Tenon’s; TNF-α, tumor necrosis factor-alpha
Treatment transitionsOf the patients who received corticosteroid eye drops as their initial treatment (line 1), 86.4% (37,869/43,850) were only treated with corticosteroid eye drops for mild NIU. The other 13.6% (5,981/43,850) subsequently switched to other treatments (line 2) (Fig. 4) and were regarded as having moderate-to-severe NIU. Some patients with moderate-to-severe NIU (42.8%, 4,468/10,449) received treatments other than corticosteroid eye drops as their initial treatment.
Fig. 4
Treatment patterns of patients with moderate-to-severe NIU in the JMDC database. Sankey diagrams showing treatment transitions in the cohort that previously received corticosteroid eye drops and were subsequently given other treatments than corticosteroid eye drops. Only nodes of n = ≥10 are shown. CS, corticosteroid; JMDC, Japan Medical Data Center; NIU, non-infectious uveitis; Tx, treatment
Treatment transitions: systemic corticosteroidsFor patients with moderate-to-severe NIU receiving oral corticosteroids at least once during the study period (71.5%, 7,473/10,449), 83.7% (6,257/7,473) of patients were started on oral corticosteroids alone or in combination with corticosteroid eye drops (Fig. 5A). Among these 6,257 patients, 3,331 (53.2%) subsequently transitioned to corticosteroid eye drops, and 2,707 (43.3%) were censored. The remaining 219 patients (3.5%) required other treatments (only treatments given to groups of ≥ 10 patients are shown). In patients who switched to corticosteroid eye drops alone after oral corticosteroids (44.2%, 3,303/7,473), 74.7%, 12.2%, and 13.1% were treated with oral corticosteroids for < 1 month, ≥ 1 month to < 3 months, or ≥ 3 months, respectively, before switching. In patients who switched to censor after oral corticosteroids (33.1%, 2,477/7,473), 45.2%, 12.1%, and 42.7% of patients were treated with oral corticosteroids for < 1 month, ≥ 1 month to < 3 months, or ≥ 3 months, respectively, before switching. During the first year of treatment, 13.0% (1,358/10,449) of patients with moderate-to-severe NIU were on high-dose oral corticosteroids (≥ 7.5 mg/day) (Table 2), which decreased to 2.6% (193/7,441) during the second year of treatment.
Fig. 5
Treatment patterns in patients with moderate-to-severe NIU receiving systemic corticosteroids. Sankey diagrams showing treatment transitions before and after initiation of corticosteroids via (A) oral administration and (B) intravenous infusion. Only nodes of n = ≥10 are shown. Col, colchicine; CS, corticosteroid; inj, injection; IS, immunosuppressant; IV, intravenous; M0; no previous treatment; NIU, non-infectious uveitis; SCJ, subconjunctival; ST, sub-Tenon’s; TNF-α, tumor necrosis factor-alpha
Table 2 Steroid treatment burden in patients with moderate-to-severe NIUFor patients receiving a corticosteroid drip infusion (intravenous injection, 10.7%, 1,117/10,449), patients were mostly given intravenous corticosteroids either alone or in combination with oral corticosteroids (87.7%, 980/1,117) (Fig. 5B). Although many of these patients switched from corticosteroid eye drops to intravenous corticosteroids, the majority of patients subsequently switched away from intravenous corticosteroids to either oral corticosteroids or corticosteroid eye drops (61.4%, 602/980).
Treatment transitions: local corticosteroid injectionsFor patients with moderate-to-severe NIU who received posterior corticosteroid sub-Tenon’s injections at least once during the study period (15.7%, 1,636/10,449), patients were most commonly treated with corticosteroid eye drops before and after the sub-Tenon’s injections (Fig. 6A). In patients who switched to corticosteroid eye drops after sub-Tenon’s injections (40.8%, 667/1,636), 69.9%, 19.9%, and 10.2% received one, two, and three or more injections, respectively, before switching. In patients who switched to censor after sub-Tenon’s injections (31.7%, 519/1,636), 66.9%, 19.5%, and 13.7% received one, two, and three or more injections, respectively, before switching.
Fig. 6
Treatment patterns in patients with moderate-to-severe NIU receiving local corticosteroid injections. Sankey diagrams showing treatment transitions before and after initiation of corticosteroids via (A) sub-Tenon’s injections and (B) subconjunctival injections. Only nodes of n = ≥10 are shown. Col, colchicine; CS, corticosteroid; inj, injection; IS, immunosuppressant; M0; no previous treatment; NIU, non-infectious uveitis; SCJ, subconjunctival; ST, sub-Tenon’s
For patients with moderate-to-severe NIU receiving corticosteroid subconjunctival injections at least once during the study period (10.0%, 1,046/10,449), patients were most commonly treated with corticosteroid eye drops before and after the subconjunctival injections (Fig. 6B). In patients who switched to corticosteroid eye drops after subconjunctival injections (68.5%, 717/1,046), 66.1%, 20.4%, and 13.5% received one, two, and three or more injections, respectively, before switching.
Treatment transitions: TNF-α inhibitorsFor patients with moderate-to-severe NIU who were treated with TNF-α inhibitors at least once during the study period (313/10,449, adalimumab n = 220 or infliximab n = 108, some patients received both TNF-α inhibitors during the study period), 69.3% (217/313) of patients received concomitant medications, including systemic immunosuppressants, oral corticosteroids, and/or other treatments (Fig. 7 and Fig. S1). TNF-α inhibitors were the initial treatment in 26.2% (82/313) of patients who received TNF-α inhibitors during the study period. In patients who switched to censor after treatment with TNF-α inhibitors, 70.5% (43/61) were treated for ≥ 12 months.
Fig. 7
Treatment patterns in patients with moderate-to-severe NIU receiving TNF-α inhibitors (adalimumab or infliximab). Sankey diagram shows treatment transitions before and after initiation of TNF-α inhibitors. Only nodes of n = ≥10 are shown. Col, colchicine; CS, corticosteroid; IS, immunosuppressant; IV, intravenous; M0; no previous treatment; NIU, non-infectious uveitis; TNF-α, tumor necrosis factor-alpha
Treatment lines for NIUWe also investigated treatment lines for patients with NIU (for all treatments except corticosteroid eye drops). Posterior sub-Tenon’s and subconjunctival corticosteroid injections were most common at treatment line 1 for patients with moderate-to-severe NIU (Fig. 8), whereas systemic (oral/intravenous) corticosteroids, intravitreal corticosteroids, and immunosuppressants were most common at treatment line 2 (Fig. 8).
Fig. 8
Proportion of patients with moderate-to-severe NIU receiving treatments other than corticosteroid eye drops at each line. Inj, injection; IS, immunosuppressant; IV, intravenous; IVT, intravitreal; NIU, non-infectious uveitis; SCJ, subconjunctival; ST, sub-Tenon’s; TNF-α, tumor necrosis factor-alpha
Incidence of ocular diseases associated with NIU or its treatmentThe overall estimated incidence rate of treatment-related ocular diseases and potentially related surgeries was higher during the first year of NIU treatment (Table 3) than years 2–5 of treatment. Prescription of glaucoma drugs was common in patients with mild and moderate-to-severe NIU and was highest during the first year of treatment (estimated incidence was 106–119 per 1,000 PY at 1 year, 73–74 per 1,000 PY at 2 years, and 50–52 per 1,000 PY at 5 years). During the first year of NIU treatment, cataract surgery was more common in patients with mild NIU (52 per 1,000 PY) than in patients with moderate-to-severe NIU (31 per 1,000 PY). The incidence of prescription of glaucoma drugs, glaucoma surgery, cataract surgery, and vitreous surgery during years 1–5 of treatment was higher in patients who received posterior sub-Tenon's corticosteroid injections than in all patients with moderate-to-severe NIU. For example, estimated incidence of prescription of glaucoma drugs in patients receiving sub-Tenon's corticosteroid injections was 235 per 1,000 PY at 1 year, 166 per 1,000 PY at 2 years, and 117 per 1,000 PY at 5 years.
Table 3 Estimated (95% CI) incidence ratea of treatment-related ocular diseases and potentially related surgeries in patients with NIUUveitis-related ocular diseasesThe estimated incidence rate of UME was higher in patients with moderate-to-severe NIU (69 per 1,000 PY) than in patients with mild NIU (32 per 1,000 PY), particularly during the first year of treatment (Table 4). The estimated incidence of UME during years 1–5 of NIU treatment was also higher in patients who received posterior sub-Tenon's corticosteroid injections (260 per 1,000 PY at 1 year, 166 per 1,000 PY at 2 years, and 112 per 1,000 PY at 5 years) than in all patients with moderate-to-severe NIU (69 per 1,000 PY at 1 year, 46 per 1,000 PY at 2 years, and 32 per 1,000 PY at 5 years). The incidence of ERM generally remained unchanged during years 1–5 of NIU treatment and was higher in patients who received posterior sub-Tenon's corticosteroid injections (46 per 1,000 PY at 1 year) than in all patients with moderate-to-severe NIU (19 per 1,000 PY at 1 year).
Table 4 Estimated (95% CI) incidence ratea of uveitis-related ocular diseases in patients with NIU
Comments (0)