
Remember me




Tubulointerstitial nephritis (TIN) and uveitis was initially described by Dobrin et al. in 1975 [1]. The condition holds no specific diagnostic criteria but is defined as the occurrence of tubulointerstitial nephritis and uveitis in a patient in the absence of other systemic diseases that can cause interstitial nephritis or uveitis [2]. The exact cause of TINU is unknown but it is thought to be an autoimmune mediated event that may be related to infection, certain medications or idiopathic in nature [2].
Research has shown that the prevalence of TINU in uveitis centres is low but the syndrome is also under-diagnosed [3]. TIN in isolation is a potentially life-threatening condition and is diagnosed histologically as interstitial oedema with inflammatory cell infiltrates [4]. Patients with unexplained acute kidney injury (AKI) events or reduced estimated glomerular filtration rate (eGFR) should consider TIN as a noteworthy differential. The precise array of symptoms associated with TIN are largely non-specific. A renal biopsy is therefore required to confirm diagnosis. In addition to this, noteworthy systemic conditions must be excluded including systemic lupus erythematous (SLE), Tuberculosis (TB), sarcoidosis and Sjogren’s disease.
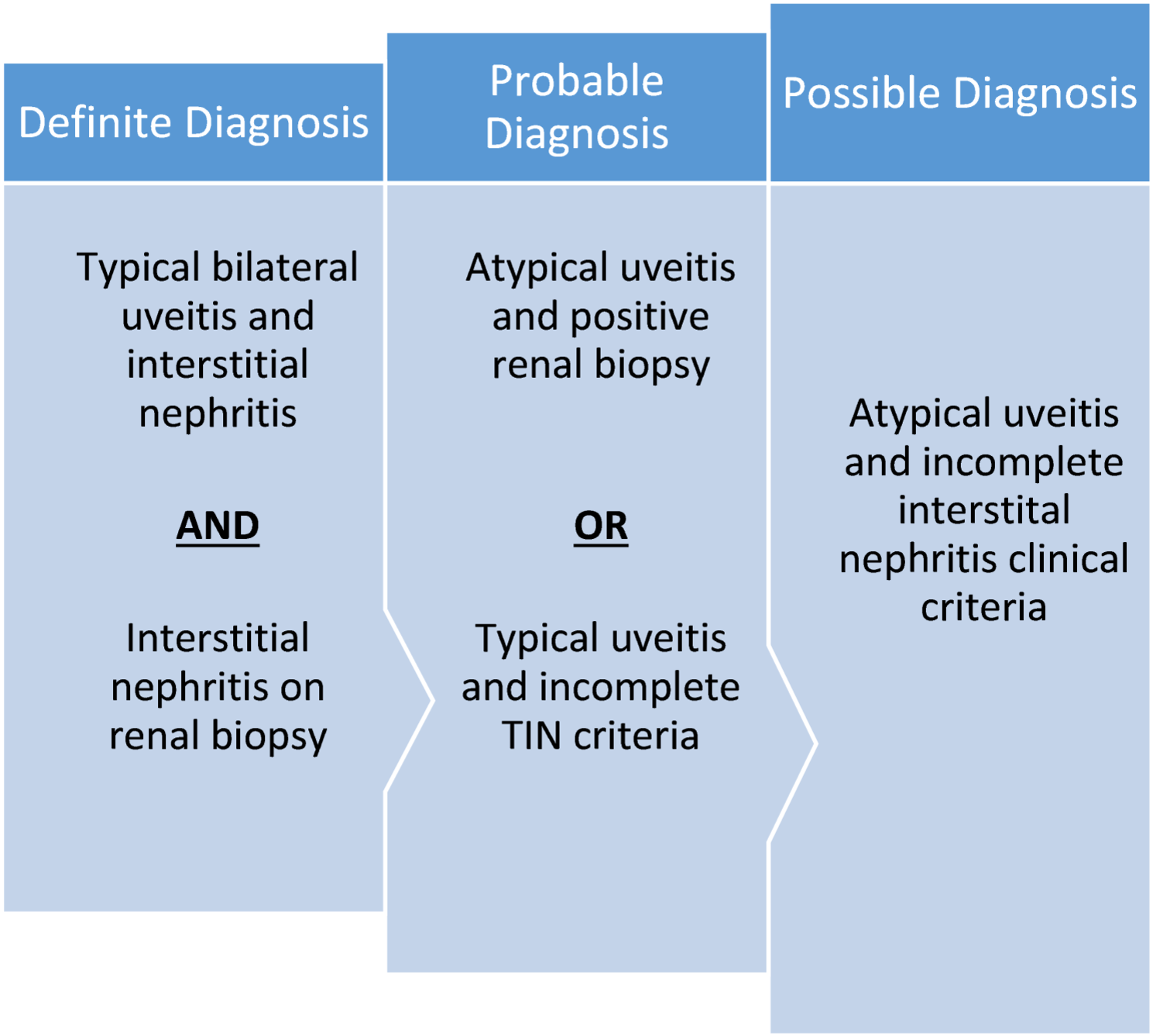
Mandeville et al. devised diagnostic criteria for the classification of patients with TINU which is illustrated in the fig. 1 shown below.
Fig. 1
Diagnostic criteria of tubulointerstitial nephritis and uveitis syndrome (TINU syndrome)
Interstitial nephritis clinical criteria
1.Abnormal renal function.
2.Abnormal urinalysis.
3.Systemic illness ≥ 2 weeks including fever, weight loss, lab abnormalities.
The purpose of this case series is to raise awareness of this rare clinical entity and to highlight the importance of screening for uveitis in patients diagnosed with interstitial nephritis in a level three hospital in the south east of Ireland. In this series, five clinical case studies of TINU syndrome are presented and clearly articulate the associated between interstitial nephritis and uveitis.
Clinical casesCase 1A 42 year old female presented to eye casualty in University Hospital Waterford (UHW) with acute bilateral red eye of 7 day duration. She gave a history significant for malaise and anorexia of one month duration with no previous episodes reported. Background history significant for asthma. She was untreated in the lead up to initial presentation.
Ophthalmology findings were significant for conjunctival injection bilaterally, inferior non-granulomatous keratic precipitates bilaterally, + 3 cells in the anterior chamber bilaterally (SUN criteria) and normal intraocular pressures. Her presenting visual acuity was 0.3 LogMAR to the right eye and 0.4 LogMAR to the left eye unaided. A diagnosis on non-granulomatous anterior uveitis was made. The SUN Working Group commenced in 2004 when 50 uveitis specialists came together to standardize the approach to classifying uveitis clinical cases [5]. A consensus on the anatomic classification was reached detailing structural components of uveitis, anterior chamber grading, anterior chamber flare and inflammation severity [5].
Laboratory evaluation showed Creatinine level of 333 µmol/L(eGFR-15 ml/min/1.73m2), urea 8.4 mmol/L, free thyroxine 19.2 pmol/L, TSH 0.062 mLU/L, Anti Thyroid Microsomal Ab-Negative, Anti Thyroglobulin Ab-Negative. Serum ACE- 33 (8–52) U/L. Urinary Protein/creatinine ratio (U PCR) − 63 mg/mmol (0–15). Anti- Nuclear Antibody (ANA)-negative, Anti DsDNA-negative, Anti-Ro/La-negative, Anti-Neutrophil Cytoplasmic Ab (ANCA) -negative.
A renal biopsy was performed following nephrology input which showed features consistent with active chronic tubule interstitial nephritis.
The presence of uveitis and TIN justified a diagnosis of TINU syndrome. Infective and systemic causes were ruled out and included: hepatitis B and C, Toxoplasma gondii, Epstein-Barr, cytomegalovirus, brucellosis, syphilis, systemic lupus erythematous (SLE), Tuberculosis (TB), sarcoidosis and Sjogren’s disease.
The patient was subsequently managed on oral steroids in the form of prednisolone (1 mg/kg/day) as monotherapy. After 2 months of commencing treatment her creatinine improved to 120 µmol/L (eGFR-50 ml/min/1.73m2). She was followed for 13 years in our nephrology clinic and had no recurrence during her follow up and was discharged from our clinic with a creatinine of 92 µmol/L (eGFR-63 ml/min/1.73m2). At this point, her visual acuity had improved to 0.2 LogMAR in the right eye and 0.3 LogMAR in the left eye.
Case 2A 57 year old gentleman presented to hospital feeling generally unwell with a red left eye associated with significant pain on eye movement. Three weeks previously he had been admitted to a level 3 hospital with night sweats, right renal angle pain and rigors. He was treated as a urinary tract infection and his antibiotic regimen included Clarithromycin and Cephalexin. His creatinine on discharge from that hospital was 206 µmol/L (eGFR-32 ml/min/1.73m2). His baseline creatinine prior to that hospital admission was 100–110 µ mmol/L (eGFR-68-76 ml/min/1.73m2). His medical history was significant for psoriasis.
Labaratory evaluation showed a Creatinine level of 181 µmol/L(eGFR-37 ml/min/1.73m2), urea 6.4 mmol/L, TSH 1.85 mLU/L. Anti- Thyroid Microsomal Ab-negative, Anti Thyroglobulin Ab.-Positive titre 1:100. ANA-Negative, ANCA-negative. U PCR-36 mg/mmol. Serum ACE-19 U/L (8 to 52). Urine- AFB negative and TB culture negative. The systemic conditions which include SLE, TB, sarcoidosis and Sjogren’s disease were ruled out.
He was seen in eye casualty and ophthalmology findings were reported as fine non-granulomatous keratic precipitates in the left corneal endothelium and + 2 cells in the anterior chamber along with left posterior synechiae. His presenting visual acuity was 0.4 LogMAR bilaterally unaided. Fundal examination was unremarkable bilaterally with no posterior segment involvement noted. A clinical diagnosis of left non-granulomatous anterior uveitis was made.
The electrolyte results prompted nephrology input with subsequent biopsy showing features consistent with severe acute tubulointerstitial nephritis. This patient was managed with oral steroids in the form of prednisolone (1 mg/kg/day). After 12 months of follow up creatinine reached a nadir of 108umol/L (eGFR-69 ml/min/1.73m2). His visual acuity had improved to 0.2 LogMAR bilaterally unaided. He was discharged from clinic following 3 years of follow up with a U PCR-15 mg/mmol and creatinine-115 µmol/L (eGFR-64 ml/min/1.73m2).
Case 3A 45 year gentleman was referred to the Acute Medical Assessment Unit with a 6 week history of ‘flu-like’ symptoms. He reported generalised myalgia; weight loss of 7 kg; night sweats, fevers and fatigue. He also reported new onset bilateral red eye, photophobia and pain affecting both eyes.
His medical history was significant for type 2 diabetes mellitus and dyslipidaemia. His medications included Metformin, Gliclazide, Sitagliptin and Pravastatin.
Initial investigations performed showed a creatinine level of 231 µmol/L (eGFR-30 ml/min/1.73m2), urea 15.6 mmol/L, free thyroxine 44.9 pmol/L, TSH 0.008 mLU/L. ANA-Pos (very weak), Anti Thyroid Microsomal Ab-Negative, Anti Thyroglobulin Ab-Negative, Anti dsDNA Ab- Negative, Anti SSA(Ro) Ab-Negative, Anti SSB(La) Ab-Negative, ANCA-negative and U PCR-51 mg/mmol.
He was subsequently reviewed in eye casualty and ophthalmology findings reported right conjunctival injection, + 3 cells in the right anterior chamber and + 1 cells in the left anterior chamber. Intraocular pressures were 6 mm Hg in the right eye and 10 mm Hg in the left eye. His initial visual acuity was 0.3 LogMAR bilaterally with glasses. Fundal exam was normal and there was no posterior synechiae noted. The posterior segment exam findings were non-contributory. A diagnosis of non-granulomatous bilateral anterior uveitis was made. The systemic conditions which include SLE, TB, sarcoidosis and Sjogren’s disease were ruled out.
A renal biopsy was performed, and it demonstrated features of active moderate acute tubulointerstitial nephritis most consistent with allergic aetiology.
He was commenced on oral prednisolone (1 mg/kg/day). His newly diagnosed hyperthyroidism was managed by our endocrinology colleagues with carbimazole 20 mg once daily orally.
He was followed up in Nephrology clinic for 4 years without any recurrence of disease and was discharged from clinic with a creatinine of 94 µmol/L (eGFR-86 ml/min/1.73m2). His visual acuity remained stable at 0.3 LogMAR bilaterally with the aid of glasses.
Case 4A 71 year old gentleman presented to the Emergency Department with a 4 week history of feeling generally unwell with nausea, fatigue, weight loss and had bilateral red eyes with photophobia. His background history was significant for type 2 diabetes mellitus, hypertension and dyslipidaemia. His ophthalmology history was significant for primary open angle glaucoma (POAG).
Laboratory findings reported a Creatinine level of 317 µmol/L (eGFR-17 ml/min/1.73m2), urea 8.5 mmol/L, free thyroxine 15.9 pmol/L, TSH 3.6 mLU/L. ANA-pos (very weak). U PCR-14 mg/mmol. HbA1c- 48 mmol/mol. The systemic conditions which include SLE, TB, sarcoidosis and Sjogren’s disease were ruled out.
He was referred to eye casualty and ophthalmology findings were relevant for bilateral conjunctival infection, + 1 cells in the right eye and + 2 cells in the left eye. His presenting visual acuity was recorded as 0.2 LogMAR in the right eye and 0.3 LogMAR in the left eye unaided. The posterior segment exam was non-contributory. These clinical findings were in keeping with a diagnosis of anterior uveitis.
He underwent a renal biopsy which demonstrated tubulointerstitial nephritis with the presence of eosinophils suggestive of allergic aetiology.
This patient was initially managed with oral steroids for 6 months using prednisolone (1 mg/kg/day) and was subsequently commenced on azathioprine (1.5 mg/kg/day). Following 3 months of commencing treatment his creatinine improved to 145 µmol/L (eGFR- 44 ml/min/1.73m2). The most recent visual acuity was recorded as 0.2 LogMAR bilaterally unaided. This patient was followed up in nephrology clinic until he passed away 4 years later.
Case 5A 59 year old gentleman was referred to nephrology clinic with a rise in his serum creatinine 160 µmol/L (eGFR-43 ml/min/1.73m2) noted 3 months previously by his GP. He had a previous baseline creatinine of 70–90 µmol/L (eGFR-85-102 ml/min/1.73m2). He denied any constitutional symptoms and reported he otherwise felt well. He had a history of venous thromboembolism (VTE) with weak positive anti-phospholipid antibody tests and was commenced on warfarin approximately two years previously.
Laboratory results showed a creatinine level of 160 µmol/L (eGFR-43 ml/min/1.73m2), urea 7.6 mmol/L, free thyroxine 14.3 pmol/L, TSH 5 mLU/L. HBs Ag-Not Detected, Anti-HCV-Not Detected, HIV Ag/Ab -Not Detected, Urinary Albumin/Creatinine Ratio-25 mg/mmol (0.0 to 2.5), ANA- Pos (very weak), Anti- Proteinase 3 Ab -negative, Anti Myeloperoxidase Ab-negative, Anti GBM Ab-Negative.
He had a renal biopsy performed which demonstrated low grade interstitial nephritis. His anticoagulation was changed to apixaban prior to renal biopsy for ease of management. The systemic conditions which include SLE, TB, sarcoidosis and Sjogren’s disease were ruled out.
At a subsequent clinic appointment, on receipt of renal biopsy results, it was noted that he had bilateral red eyes. The patient had been attending our Nephrology clinic for 6 months at this point. He also reported that this symptom had been ongoing for approximately 2 years and he attributed it to occupational exposure to dust.
He was reviewed in eye casualty and ophthalmology findings were significant for bilateral conjunctival injection with + 0.5 cells in the right anterior chamber and + 2 cells in the left anterior chamber. Intraocular pressures were 23 mm Hg in the right eye and 20 mm Hg in the left eye. His initial visual acuity was 0.4 LogMAR in the right eye and 0.3 LogMAR in the left eye.There was no posterior synechiae noted and fundal exam was non-contributory. The posterior segment exam was unremarkable. A diagnosis of bilateral anterior uveitis secondary to tubulointerstitial nephritis was made. The patient was treated with topical steroids and a cycloplegic agent and showed an improvement in symptom control and anterior chamber activity at the two week follow-up period. The final visual acuity was 0.2 LogMAR bilaterally following steroid treatment.
He has been managed with oral steroid prednisolone (1 mg/kg/day) in the Nephrology clinic. His most recent creatinine was 148mmol/L (eGFR-47 ml/min/1.73 m²) which was 6 weeks after commencing therapy.
Comments (0)