Participants
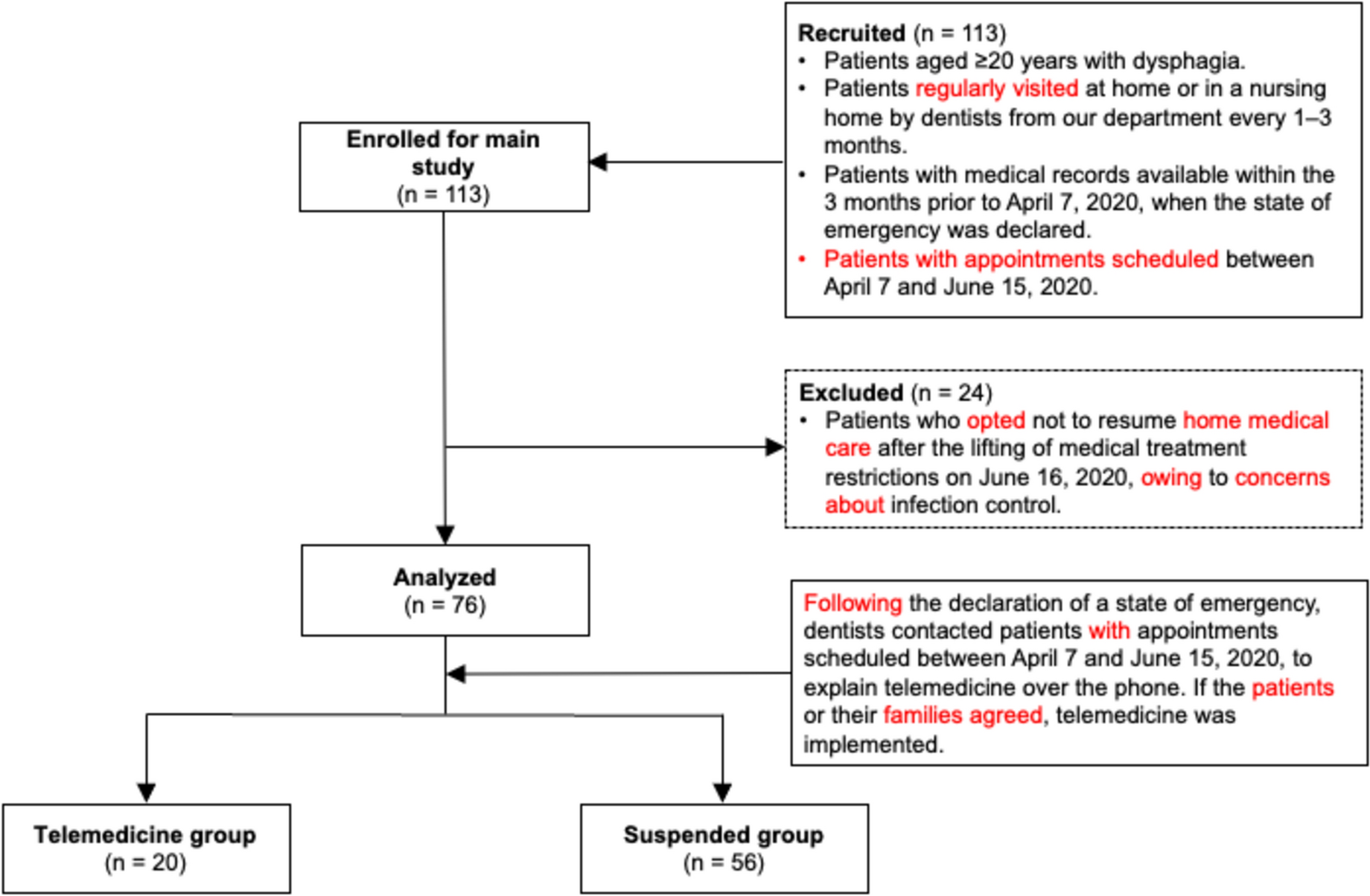
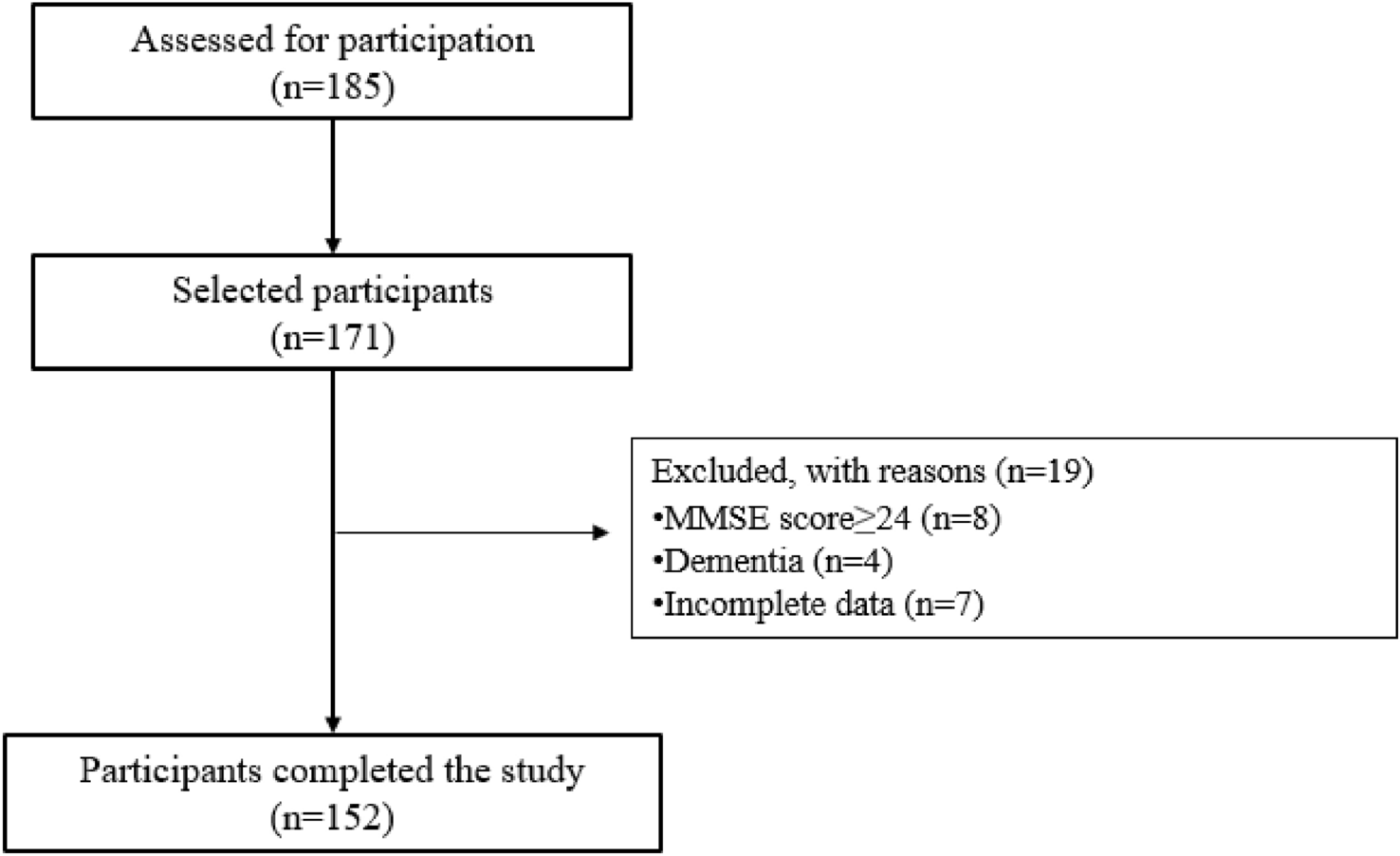
Patients with dysphagia aged ≥ 20 years, who were regularly visited at home or in a nursing home by dentists from our department every 1–3 months, were included in this retrospective study. Dysphagia was evaluated by dentists in our department. Patients with medical records from the 3 months preceding the declaration of the state of emergency on April 7, 2020, and with appointments scheduled between April 7 and June 15, were selected. Before the suspension of HMC, swallowing endoscopy was performed every 1–3 months during face-to-face visits. Based on examination results, patients were instructed on the appropriate dietary form, swallowing training, and environmental settings for eating and training. The frequency of face-to-face visits was determined by the dentist in charge based on the patient’s condition. After the suspension of face-to-face visits, telemedicine was explained to patients via telephone and provided if they or their family members opted for it. The dentist in charge also determined the frequency of telemedicine consultations, and all patients who received telemedicine complied. Patients who declined telemedicine had their treatment suspended until June 15, 2020, when restrictions on medical treatment at our hospital were lifted, and face-to-face care was resumed. The exclusion criteria included patients who, after the lifting of restrictions, declined to resume HMC owing to concerns about infection control.
Intervention
Telemedicine was implemented from April 7, 2020, to June 15, 2020, during the suspension of the hospital’s clinic system. Patients and the hospital were connected via mobile phones with camera functions, PCs, tablets, and other information and communication devices. An online information system called YaDoc (Integrity Healthcare Co., Ltd., Tokyo, Japan), a telemedicine application that encrypts medical information and communication, was used. On the patient side, connections were facilitated by patients themselves or telemedicine supporters, such as family members, caregivers, or healthcare professionals. The YaDoc application was selected for its user-friendly interface and robust focus on protecting personal information. The dentist provided instructions on downloading and using the YaDoc application to the patient or telemedicine supporters via phone or email. No prior training or preparation was required for either dentists or patients in using YaDoc. No pilot test or trial period was needed, and no modifications were made to the YaDoc application during the study. Before starting the telemedicine consultation, the dentist and patient tested the connection to ensure the system was functioning properly. Each telemedicine session lasted approximately 30 min, during which the dentist interviewed the patient and observed their eating habits. Based on the interview findings and the patient’s eating habits, the dentist provided guidance on compensatory techniques, as well as direct and indirect therapies. Specifically, compensatory techniques included adjustment of dietary forms, eating environments, and posture during meals. Direct swallowing therapy involved various exercises such as swallowing practice with thickened water or jelly and chewing practice using snack foods. Indirect swallowing therapy included oral motor exercises, strengthening exercises for swallowing-related muscles such as the suprahyoid muscles, and respiratory rehabilitation. Additionally, instructions were provided on nutritional management, oral hygiene, and the use of oral protective mouthpieces. Eating habits were classified into the following three categories: independent oral intake (self-intake of meals), assisted oral intake (with caregiver support), and oral intake practice (small quantities of food consumed for practice when primary nutrition was provided non-orally). The content of each group’s intervention is categorized into Evaluation/Assessment and Instructions/Treatment, as detailed in Table 1. The frequency of online visits was determined using the same criteria as for the previously conducted home visits. The dentist made decisions comprehensively based on clinical findings, including the severity of dysphagia, the presence of aspiration or laryngeal penetration observed during video endoscopy examination, the risk of aspiration pneumonia, the patient’s nutritional status, and the level of concern expressed by the patient or their family regarding swallowing function. When clinical findings indicated a higher risk, the frequency of visits was set at 1–2 times per month. If the clinical condition was stable, the interval between visits was extended to more than 2 months. Telemedicine was provided by the same dentist who had been conducting face-to-face visits before the COVID-19 pandemic. All participating dentists had at least 10 years of clinical experience in dysphagia rehabilitation.
Table 1 Contents of telemedicine consultOutcomes
Basic participant information, including age, sex, body mass index (BMI), primary disease, medical history, history of aspiration pneumonia, activity status, and the Charlson Comorbidity Index (CCI) [17], was collected from medical records as of April 1, 2020. The Barthel Index (BI) score [18] was obtained to assess the patient’s activity status. Oral intake status was evaluated using the Functional Oral Intake Scale (FOIS) [19], which has the following seven levels: 1 = no oral intake; 2 = tube-dependent with minimal/inconsistent oral intake; 3 = tube supplements with consistent oral intake; 4 = total oral intake of a single consistency; 5 = total oral intake of multiple consistencies requiring special preparation; 6 = total oral intake with no special preparation but avoidance of specific foods or liquids; and 7 = total oral intake with no restrictions [19]. Baseline dysphagia severity was assessed using the Dysphagia Severity Scale (DSS), based on swallowing endoscopy performed within 3 months before the suspension of HMC. The DSS is a seven-point scale, with lower scores indicating more severe dysphagia [20]. Data were also collected on the primary provider of dysphagia care and whether healthcare professionals, including home care nurses, speech-language pathologists, and dental hygienists, provided interventions for dysphagia. Additionally, the number of days between the last face-to-face medical care before the suspension of home visits and the resumption of face-to-face care was calculated.
We retrospectively assessed the number of adverse events related to whole-body conditions or dysphagia that occurred between April 7, 2020, and June 15, 2020, during the suspension of our clinic system and home visits. Adverse events related to whole-body conditions were defined as follows: (1) death during the suspension period, regardless of the cause, and (2) hospitalization during the suspension period, regardless of the underlying disease. Adverse events related to dysphagia were defined as follows: (1) aspiration pneumonia, diagnosed by the attending physician; (2) choking, characterized by symptoms of airway obstruction with food; and (3) decline in swallowing function, identified by coughing when food or liquids approached the airway, prolonged mealtime exceeding 10 min since the last face-to-face visit, or weight loss of > 5% of baseline body weight owing to reduced food intake. Choking and decline in swallowing function were directly assessed by the dentist through interviews with the patient or caregiver during the first resumed visit after June 16, 2020. If a patient’s medical record contained information meeting any of these criteria, it was classified as a dysphagia-related adverse event.
Statistical Analysis
The participants were categorized into the following two groups: those who received telemedicine (telemedicine group: TG) and those who did not and were suspended from receiving HMC (suspended group: SG). Statistical analysis was conducted to determine whether differences existed between the TG and SG regarding basic participant information and the incidence of adverse events. Continuous variables, including age, BMI, BI, FOIS, DSS, and the number of days of suspended face-to-face medical care, were analyzed using the Mann–Whitney U or t-test, with normal distribution confirmed using the Shapiro–Wilk test. Categorical variables, such as sex, medical history, history of aspiration pneumonia, and incidence of adverse events, were analyzed using Fisher’s exact test.
Factors associated with dysphagia-related adverse events were also examined. Patient characteristics were compared based on the presence or absence of dysphagia-related adverse events. Using univariate analysis, dysphagia-related adverse events were set as the dependent variable, and all survey items were treated as independent variables to calculate crude odds ratios and 95% confidence intervals. Binomial logistic regression analysis was performed to adjust for confounding factors, with dysphagia-related adverse events classified into the following two groups: with and without dysphagia-related adverse events. Telemedicine implementation, age, CCI, and DSS were selected as independent variables. Age was adjusted as it is associated with dysphagia [21], and CCI was included owing to significant differences observed between TG and SG. DSS, reflecting the clinical severity of dysphagia, was incorporated as a predictor of adverse events. DSS scores (1–4: aspiration present; 5–7: aspiration absent) were divided into these categories owing to the significant impact of aspiration on dysphagia outcomes. Statistical significance was set at 5%. Analyses were conducted using IBM SPSS Statistics for Windows, version 28.0.1.1 (IBM Corp, Armonk, NY, USA).




Comments (0)