
Remember me



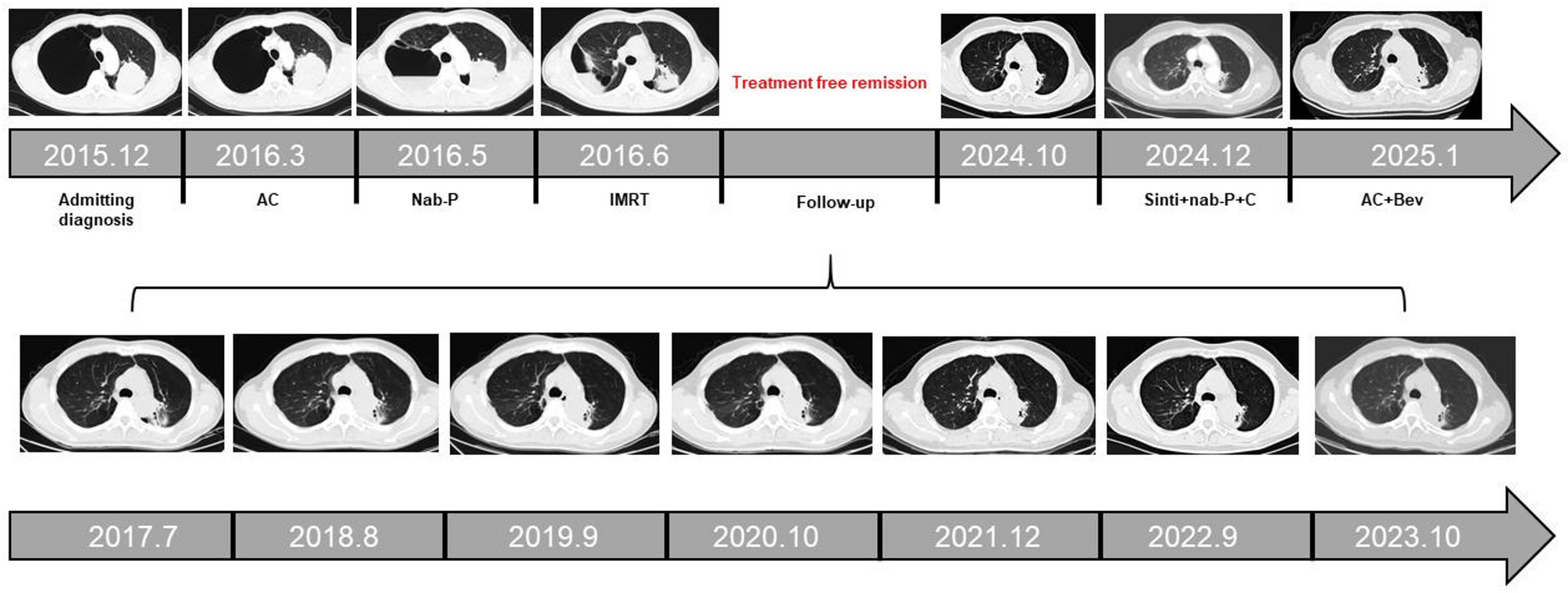

A 59-year-old male patient presented to our hospital on December 2, 2015, with a six-month history of cough and chest tightness. He had no history of smoking. Initial chest imaging at an outside hospital revealed a mass in the left upper lung with concomitant bullous lung disease. Upon admission, the patient’s ECOG performance status was 1. Chest CT showed left upper lobe bronchial stenosis with a lobulated soft tissue mass, approximately 7 cm in size. Additionally, mediastinal and hilar lymph nodes (stations 5, 6, 7, 10 L, and 11 L) were enlarged. Brain MRI and abdominal CT did not show any distant organ metastases. A PET-CT scan was also performed at the time of diagnosis. It demonstrated increased FDG uptake in the left upper lobe mass (SUVmax = 5.23), as well as in the left hilar (SUVmax = 2.60) and mediastinal lymph nodes (SUVmax = 2.10), without distant metastases. Based on the 7th edition TNM staging system, the patient was diagnosed with cT3N2M0, corresponding to stage IIIB lung cancer. The percutaneous lung biopsy confirmed the diagnosis of lung adenocarcinoma, and genetic testing showed negative results for both EGFR and ALK mutations.
Although concurrent chemoradiotherapy is the standard of care for stage IIIB NSCLC, the patient initially declined radiotherapy, believing that systemic chemotherapy alone would suffice to control the disease. The patient began two cycles of pemetrexed plus carboplatin on December 12, 2015, as first-line chemotherapy. However, on February 3, 2016, he was re-admitted due to worsening cough. Follow-up chest CT showed intrapulmonary metastasis, obstructive pneumonia, and further enlargement of mediastinal lymph nodes, indicating progressive disease (PD). On March 7, 2016, the patient commenced three cycles of nab-paclitaxel treatment. Subsequently, on May 10, 2016, he underwent left lung tumor radiotherapy with 6 MV X-rays using intensity-modulated radiation therapy (IMRT), delivering a total planned dose of 58.5 Gy. On June 2016, he received three cycles of nab-paclitaxel treatment.
The patient received thoracic radiotherapy using intensity-modulated radiation therapy (IMRT) with 6 MV X-rays. The prescribed total dose was 58.5 Gy, delivered in 26 fractions of 2.25 Gy once daily, five days per week. The clinical target volume (CTV) included the primary tumor and involved hilar and mediastinal lymph node regions. A respiratory gating technique was not applied due to patient-related limitations. No radiation-related toxicities were observed.
After regular follow-up, a CT scan on October 23, 2024, revealed local tumor progression, with an increase in the size of the treated lesion. Although the lesion remained localized, it was situated within the prior radiation field and in close proximity to critical thoracic structures. Therefore, stereotactic re-irradiation was not recommended due to concerns over cumulative radiation toxicity. The patient was instead managed with active surveillance and symptomatic treatment, with re-irradiation considered as a contingency for future localized progression. In December 2024, the patient underwent two cycles of Sintilimab combined with nab-paclitaxel and carboplatin; however, the disease progressed rapidly (Fig. 1). Subsequently, a new systemic regimen consisting of pemetrexed (950 mg, d1), carboplatin (650 mg, d1), and bevacizumab (500 mg, d1) was initiated in February 2025. The patient completed four cycles of this regimen between February and May 2025. Symptomatic improvement, including reduced chest tightness, was noted, and the treatment was well tolerated, with only mild nausea and transient headache reported.
Fig. 1
Longitudinal treatment timeline and chest computed tomography follow-up. The horizontal axis represents the clinical course from initial diagnosis (December 2015) to the last follow-up (January 2025)
Follow-up imaging revealed progressive disease, primarily involving the previously irradiated site in the left upper lobe. As of the latest follow-up in May 2025, the patient remained alive with stable general condition (ECOG 1), normal appetite, sleep, and bowel/bladder function, and no significant weight loss.
Histopathological analysis of baseline tumor slide identified malignant characteristics in the lung tumor, including disrupted tissue organization (6.8×) and pleomorphic nuclei with prominent nucleoli (16.3×) on H&E staining (Fig. 2).
Fig. 2
Histopathological analysis of lung tumor biopsy specimens by hematoxylin and eosin (H&E) staining. (A) Low-magnification view (6.8×) showing overall tumor architecture. (B) High-magnification view (16.3×) revealing cytological details
Peripheral blood samples in November 2024 were collected for single-cell RNA sequencing. After dimensionality reduction and cluster analysis, we obtained 15 peripheral blood components (Fig. 3A) and their respective proportions (Fig. 3B). Immune cells had been grouped 14 different cell clusters which were respectively annotated by markers (Fig. 3C). Notably, the patient exhibited a high proportion of NK cells (11.58%), suggesting enhanced anti-tumor immunity. The elevated NK cell populations further support a robust and sustained innate immune response against the tumor.
Fig. 3
Single-cell RNA sequencing analysis of peripheral blood samples. (A) UMAP visualization of 15 distinct immune cell populations. (B) Proportional composition of major cell types. (C) Representative marker genes for each cell cluster. (D) Cellular interaction network frequencies of NK cells with other immune subsets. (E) Top 10 differentially expressed genes across 5 clusters. (F) Functional enrichment of signature genes in 5 clusters. (G) Kaplan-Meier survival analysis stratified by high vs. low expression of 10 prognostic signatures in cluster 1
The interaction between NK cells and neutrophils exhibited the highest frequency (Fig. 3D) and interaction weight (Supplementary Fig. 1). Further, we extracted NK cells and separated them into five clusters. The top 10 highly expressed genes were shown in the heatmap (Fig. 3E). The pathway enrichment analysis demonstrated the specific functions of each cluster. Toll-like receptors signaling pathway was enriched in cluster 0 and 1 (Fig. 3F). Finally, the signatures were composed of the top 10 genes in each cluster. High expression of signatures in cluster 1 showed a good prognosis in TCGA-LUAD dataset while the signatures in other clusters did not separate the survival curves (Fig. 3G, Supplementary Fig. 2).
Paired tumor biopsy specimens (obtained at baseline and in November 2024) were subjected to Genomic and epigenomic sequencing to identify potential molecular correlates of clinical outcome. PredicineCARE [2, 3] (Predicine) NGS analysis showed that many common genes like EGFR, ROS1, ERBB2 genes were copy number gained while MYC, PTEN, JAK2, TP53, KEAP1, CDKN2A, CDKNA2B genes were copy number loss (Supplementary Fig. 3). Furthermore, deletion of the PDCD1LG2 gene, which encodes PD-L2, an alternative ligand of the PD-1 receptor—was identified. This genetic alteration may be associated with the negative PD-L1 immunohistochemical staining (tumor proportion score < 1%) and could further contribute to the observed lack of response to immune checkpoint blockade in this patient. Genome-wide methylation profiling using PredicineEPIC [4, 5] identified 2,267 differentially methylated fragment regions (DMFRs) localized within gene promoter regions. Gene Set Enrichment Analysis (GSEA) demonstrated significant enrichment of DMFRs in biological process of GOBP_INNATE_IMMUNE_RESPONSE_ACTIVATING_CELL_SURFACE_RECEPTOR_SIGNALING_PATHWAYS (P value < 0.05, Supplementary Fig. 4).
Comments (0)