Our pooled analysis revealed significant differences in the AE profiles between BCMA-targeting and GPRC5D/FcRH5 BsAbs. These findings are crucial for optimizing patient management, counseling for side effects, and therapy selection for patients who have failed multiple lines of treatment. The main AEs were hematologic, infections, CRS, and neurotoxicity. The safety analysis revealed distinct AE profiles between BCMA and GPRC5D/FcRH5 BsAbs. While hematologic toxicities (e.g., neutropenia, anemia) and infections were more frequent with BCMA-directed therapies, GPRC5D/FcRH5 agents showed higher rates of CRS. The Talquetamab-containing combination group had the highest overall AE burden but the lowest grade 3/4 anemia.
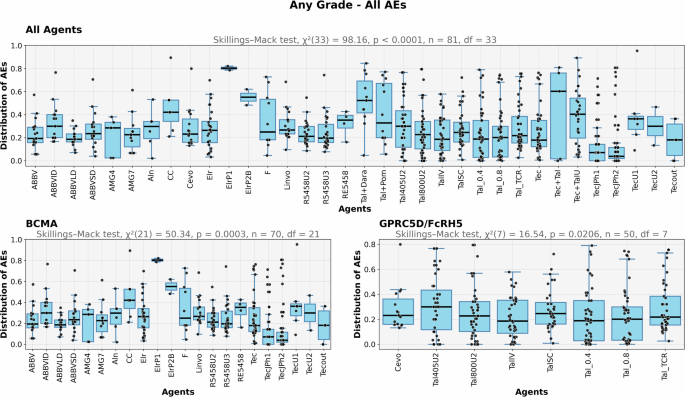
From the pooled analysis Figs. 1 and 2, we conclude that the BCMA group shows more variability and higher responses in certain agents compared to the GPRC5D/FcRH5 group. Across all plots, the generalized Friedman test indicates statistically significant differences in responses among agents. Agents with higher medians or larger spread might warrant further investigation for their effectiveness or variability. The differences between BCMA and GPRC5D/FcRH5 groups suggest that BCMA agents may be more potent or sensitive but with greater variability in their effects. GPRC5D/FcRH5 agents may offer more predictable and consistent outcomes, potentially making them preferable for scenarios requiring stability. Agents with separated from the rest or wide distributions could be explored further to understand their unique impact or variability.
Also, Fig. 3 highlights distinct clustering patterns among agents based on AE profiles. Notably, combination therapies such as Tec + Tal, Tal + Dara, and Tal + Pom form well-separated clusters, likely reflecting their unique pharmacological profiles and combined immunomodulatory effects. These agents target multiple mechanisms simultaneously, which may explain their distinct AE signatures and clustering behavior. In contrast, a couple of agents appear isolated from their expected group clusters. TecJPh2, for instance, separates from its counterpart TecJPh1, which demonstrates a substantially higher proportion of reported deaths (27% vs. 0%) and a significantly lower incidence of t(4;14) translocation (0% vs. 36%). TecJPh2 also shows approximately one-third the reporting frequency for insomnia, high-risk cytogenetics, and neurotoxicity, while exhibiting about 2.5-fold higher reporting ratios for hypogammaglobulinemia and nasopharyngitis. Another separation, Tal_TCR, includes patients previously exposed to T-cell redirection therapies and subsequently treated with the recommended subcutaneous talquetamab doses, 0.4 mg/kg weekly (Tal_0.4) or 0.8 mg/kg biweekly (Tal_0.8) [29]. Tal_TCR shows 17% stomatitis and upper respiratory tract infection vs only 1% Tal_0.4, 12% vs 1% for back pain and hypotension, and 10% vs 1% for increased alanine aminotransferase. Hypokalemia and steroid-treated CRS were approximately four times more frequent in Tal_TCR compared to Tal_0.4. Conversely, grade 3/4 fatigue and ICANS were reported at roughly one-third the frequency observed in Tal_0.4. Lastly, a comparison of ABBVID and ABBVLD reveals that ABBVID is associated with 20% CR rates vs 2% for ABBVLD. In addition, CRS, vomiting, neutropenia, lymphopenia, grade 3/4 neutropenia, ORR, nausea, anemia, and diarrhea are reported approximately twice as frequently in ABBVID. Conversely, ABBVID shows about four times lower PR rates and roughly half the incidence of death compared to ABBVLD.
Hematologic AEs, particularly cytopenias (leukopenia, thrombocytopenia, and anemia) were observed at high rates across both BCMA and GPRC5D/FcRH5 BsAbs. These cytopenia AEs are mostly seen with the use of BsAbs during the first treatment cycle2. Grade 3/4 neutropenia occurred in 35.17% of patients, which poses a significant risk for infection, and in many cases dose modifications, and close monitoring of febrile neutropenic episodes, supportive care interventions such as granulocyte colony-stimulating factor (G-CSF) administration in certain cases. Moreover, a recent pooled analysis found higher rates of grade 3-4 hematologic toxicities in BCMA-targeting agents, than their counterparts. Similar trends were observed in our study, as grade 3-4 neutropenia and anemia were most frequently reported in patients receiving teclistamab and elranatamb. These complications, namely neutropenia-related infections, can be potentially life-threatening and result in treatment delays and dose reductions, which in turn can affect treatment efficacy [40].
Infections (45.75%) demonstrated distinct patterns across treatment groups, with the highest all-grade incidence occurring in talquetamab-containing combinations, followed by BCMA×GPRC5D BsAbs. Notably, single-target BCMA agents showed higher infection rates (45.3% all-grade, 21.63% grade 3-4) compared to GPRC5D/FcRH5 therapies (42.57% all-grade, 14.51% grade 3-4). This finding likely reflects both the concurrent expression of BCMA on mature B cells and plasma cells and the T-cell exhaustion resulting from constant immune stimulation [41]. The constant stimulation of T-cells by these agents can also cause T-cell exhaustion and lead to the dampening of T-cell-mediated immunity [41]. This observation highlights the need for infection prophylaxis, especially in patients receiving long-term BsAbs therapy. These include the implementation of prophylactic antimicrobial agents including antiviral and PJP prophylaxis, intravenous immunoglobulin (IVIG) (3.62) replacement therapy, and vigilant monitoring for early signs of sepsis. Furthermore, it was shown that MM patients are at high risk of severe COVID-19 (3.71) infection and related mortality, especially in the setting of BCMA-targeted therapies. This highlights the vulnerability of MM patients, especially those on anti-BCMA agents to viral infections, which would influence infection control measures and vaccination decisions [42].
CRS, a well-documented AE of BsAbs, was observed in up to 64.95% of patients. CRS arises from robust activation of cytotoxic T-cells and the release of inflammatory cytokines. It can manifest with a wide spectrum of presentations, ranging from mild, flu-like symptoms, such as fatigue, headache, and myalgias; to severe, life-threatening symptoms, such as hemodynamic instability, disseminated intravascular coagulation (DIC), and multi-organ system failure [43]. In various bispecific antibody trials, all-grade CRS has been reported in 28–89% with median 71.5% of patients, while grade 3 or higher CRS incidence rate was lower (0–7%) with median 1% but for GPRC5D/FcRH5 agents CRS grade 3/4 were reported at 1.66%.
BCMA-targeting agents were associated with fewer CRS events (56.82%) as compared to GPRC5D/FCRH5-targeting agents (73.13%), and combinations (BCMA × GPRC5D: 79.62%, Tal + Dara: 77%). Most CRS events occur after the first full dose. To mitigate this risk, careful monitoring, step-up dosing with premedication, and the judicious use of steroids (6.91), tocilizumab (24.14), and dose delays have been recommended. Prophylactic administration of a single dose of tocilizumab has significantly reduced CRS incidence without affecting treatment efficacy, as demonstrated in a sub-cohort of the MajesTEC-1 study [44]. The ability to effectively manage CRS is pivotal in expanding the use of BsAbs in the outpatient setting without affecting the treatment regimen [40].
ICANS (3.96), though less frequent than CRS (64.95), remains a well-documented complication of CAR T cells and BsAbs. The incidence of ICANS, commonly presenting as mild to moderate confusion and dysgraphia, was more common in GPRC5D/FCRH5-targeting agents, namely talquetamab. Given the potential for ICANS to impact a patient’s quality of life, early identification and management of this toxicity are essential. Corticosteroids are the first line treatment for ICANS, with the addition of tocilizumab in patients with ICANS co-occurring with CRS [32].
Distinct toxicity profiles of BCMA and GPRC5D/FcRH5 BsAbs offer opportunities for personalized treatment. BCMA-targeting agents, namely teclistamab and elranatamab, present with higher hematologic and infection risks, and may require closer monitoring and prophylactic measures. Conversely, GPR5CD-targeting agents are more likely to be associated with CRS. In Phase 2 studies, skin-related AEs were reported in 69%, nail-related AEs (61%), and dysgeusia (61%). These unique on-tumor-off target toxicities are distinct and usually not severe and rarely need treatment discontinuation. However, these side effects can negatively affect the quality of life and pose potential challenges for therapy selection for relapse/relapse MM [30].
Clinical implications
Our study provides an analysis of safety and efficacy from the pooled analysis. We have learned that the use of prophylactic IVIG has significantly reduced the risk of infections in patients receiving bispecific antibodies [45]. For high-grade neutropenia, G-CSF can be safely utilized after stepping up dosage. Similarly, erythropoiesis-stimulating agents (ESAs) can be used for Hb <10 g/dl, while thrombopoietin-mimetics should be considered selectively for severe thrombocytopenia [46]. Grade 2 or higher CRS can be treated with tocilizumab 10 mg/kg every 8 hours with or without dexamethasone 10 mg every 6 hours. ICANS is managed with dexamethasone 10 mg every 6 hours and then tapered down upon symptom improvement [47]. For prolonged grade 3 or 4 ICANS, it is recommended to add Anakinra 100-200 mg every 8 hours in addition to steroids [47].
Regarding dysgeusia, we did not identify any successful approaches in our pooled analysis to mitigate these side effects, however, real-world data suggest decreasing the frequency of talquetamab to q4w and prophylactic use of dexamethasone mouth rinses and nystatin mouthwash or zinc and vitamin B complex may be effective strategies to alleviate oral symptoms [48].
Our analysis provides a comprehensive assessment of standardized adverse events reporting and can inform future studies focusing on specific adverse events like skin, hair or nail toxicities or taste alterations from talquetamab as well as efforts to control increase rate of infections and strategies to employ different dosing and/or fixed duration of treatment of BCMA and non BCMA bispecific Abs. Our findings further underscore the dynamic nature of bispecific antibody research in multiple myeloma and highlight the importance of continuous data synthesis like collaborative Individual patient data (IPD) studies to enable propensity matching and adjust for confounders including prior treatment intensity or comorbidities, a limitation inherent to our current aggregated data. We believe these steps will bridge the gaps identified in this study while advancing the field toward personalized therapeutic selection.
Limitations
Our analysis faced limitations due to a significant number of unreported missing values in the underlying studies and a lack of access to patient-level data. This shortage of data prevented the use of multivariate or propensity score-matched analyses to adjust for potential confounders. In their place, we applied non-parametric methods—specifically the Skillings-Mack test and Wilcoxon Signed-Rank test—to handle missing and unbalanced data while accounting for inter-trial variability. These methods align with current best practices for meta-analyses using aggregated data and allow us to conduct robust group comparisons without relying on parametric assumptions. Nonetheless, we recognize that these approaches cannot fully control for confounding, and we highlight the need for future analyses using individual-patient-level data.
Also, some studies, especially those focused on infection-related AEs, either omitted or did not fully report these details, leading to many missing values. Additionally, some studies, driven by specific goals, neglected to report essential details, concentrating only on efficacy and a few AEs. Many abstracts also reported retests of other publications without providing baseline characteristics, further contributing to missing values in our analyses. Missing data poses a threat to the integrity of clinical research, potentially leading to biased results and reduced statistical power [49]. In our analysis, missing data was addressed by normalizing each agent with its total population to scale the values ranging within a similar interval, in this case between 0 and 1. Following the normalization process, we utilized the ranked matrix generated by the Skillings Mack test on our dataset, which handled all missing values.

Comments (0)