The present study represents the first investigation of MIH in Pachuca, Mexico; determining a prevalence of 12.3%, aligning with the 13.5% mean MIH prevalence reported in a 2021 systematic review of Mexican populations (Lopes et al. 2021). However, reported Mexican MIH prevalence varies widely from 6.8% to 37.7% (Medina Varela et al. 2024; Navarrete Esquivel 2016), reflecting the global variability in MIH prevalence values, which range from 0.48 to 46.6% (Sluka et al. 2024). The differences in diagnostic criteria, examiner experience, sampling methods (random, convenience, stratified, etc.) and socioeconomic and geographical factors such as age, gender, social position, access to healthcare for mother and child and geographical location putatively contribute to these discrepancies (Schwendicke et al. 2018; Sluka et al. 2024). The studies conducted in school settings or dental clinics may show differences in prevalence because variability in the ability of the population to access and utilise educational and/or oral health services and create a sample bias.
Demarcated hypomineralised lesions in other permanent teeth (HOPT) were detected in 23 participants (4.1%); being the second premolar most commonly affected, which contrasts with a Greek study of 1156 adolescents with 23% HOPT prevalence, predominantly affecting the second permanent molars (Kevrekidou et al. 2021). These differences emphasise the difficulties in comparing different age-related cohorts, as the present study included children aged 6–13 years limiting the number of permanent non-MIH index teeth present, compared to 14 year-olds in the Greek study where most participants would have erupted canines, second permanent molars and premolars.
Approximately half of the present participants with MIH had affected permanent incisors, compared to 36.6% in a recent systematic review (Lopes et al. 2021), which was outside the upper 95% CI of 43.7%; although several studies have reported anterior prevalence > 50%. Amongst MIH-affected FPMs, 30.6% exhibited hypersensitivity/pain, similar to the 34.7% reported in 8 year-olds in Brazil (Raposo et al. 2019), however, an even higher prevalence (45%) of hypersensitivity/pain was reported in a systematic review (Santos et al. 2024); indicating that MIH-associated pain and discomfort is a prevalent issue. Sensitivity is complex to manage successfully, with limited supporting evidence for desensitising interventions (Cavalcante et al. 2024; Hjertberg et al. 2024). Hypersensitivity can significantly impact oral hygiene practices in dental quadrants with MIH-affected FPMs, as children may avoid brushing due to discomfort, increasing their susceptibility to the development of caries lesions (in those at increased caries risk), post-eruptive breakdown and subsequent restorative care, which often has poor outcomes (Raposo et al. 2019). Given this high prevalence of hypersensitivity/pain and association with poor outcomes, oral health clinicians must prioritise early efforts to limit sensitivity via proactive intervention strategies, such as decreasing caries risk, increasing mineral gain and preventing PEB, especially in severely affected teeth, however, how to achieve this is still debatable (Cavalcante et al. 2024; Hjertberg et al. 2024).
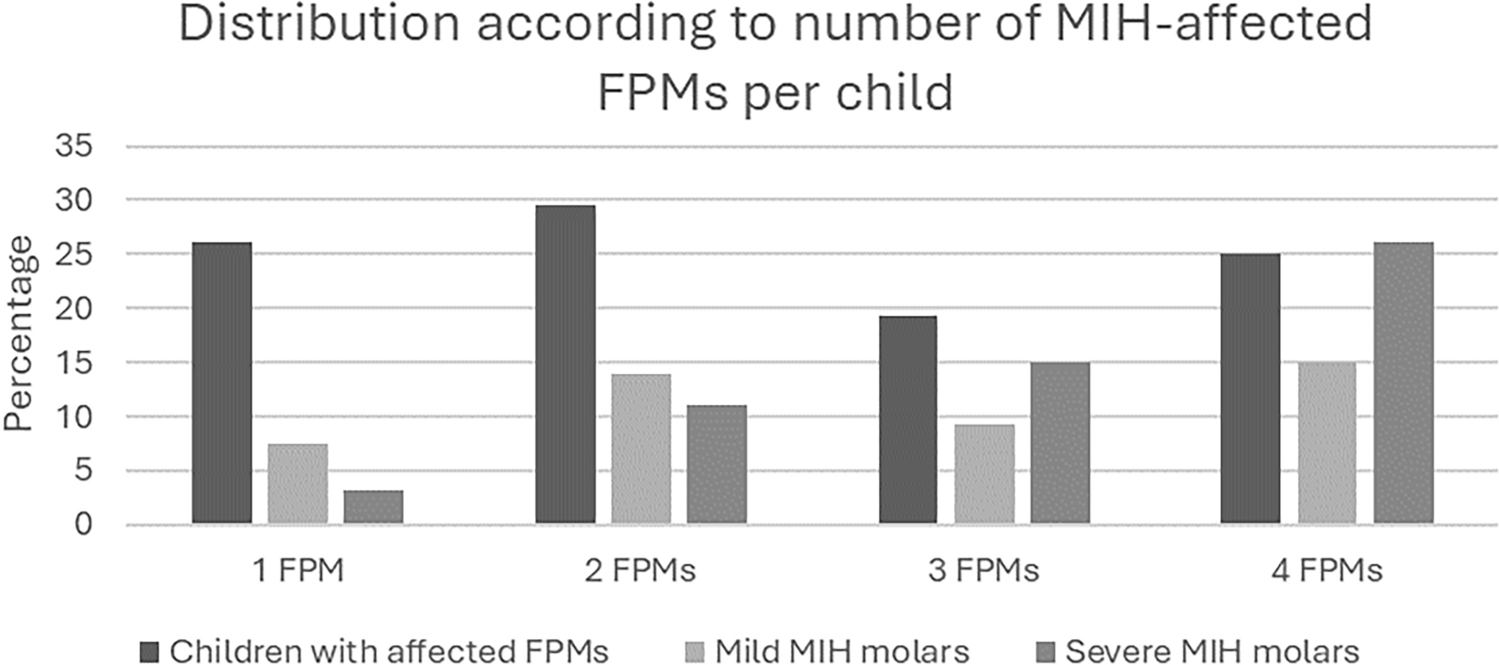
Demarcated lesions without PEB were the most common type of defect, with FPMs displaying a higher proportion of white/creamy defects compared to yellow or brown opacities. Notably, as the number of molars affected by MIH increased, lesion severity also escalated, and the number of anterior teeth affected likewise increased, echoing previous reports (Ghanim et al. 2011; Gurrusquieta et al. 2017; Sosa-Soto et al. 2022). This pattern strongly suggests a ‘dose dependent’ relationship, the greater the exposure to the aetiological factor(s) of MIH, the more teeth are affected, and the more severe the defects become (Lygidakis et al. 2008).
There was no statistically significant difference in MIH prevalence between maxillary and mandibular FPMs, with conflicting existing evidence (Abdalla et al. 2021; Ghanim et al. 2011; Preusser et al. 2007). Interestingly, in the present study, mandibular MIH-affected FPMs exhibited a higher prevalence of carious lesions, restorations and PEB, potentially due to their earlier eruption, leading to greater time exposure to occlusal forces and cariogenic environments (when present) (Wuollet et al. 2018).
Maxillary permanent incisors had a significantly higher MIH lesion prevalence than mandibular incisors, and like the FPMs, white/creamy demarcated lesions were the most common finding in incisors, consistent with other studies (Almuallem et al. 2022; Altan and Yilmaz 2023; Ghanim et al. 2011).
A notable finding on the present study is the association of MIH with father’s education level, familial structure, presence of siblings and child age. Higher socioeconomic position (SEP) appeared to be a protective factor against MIH; lower SEP may increase MIH risk and severity potentially due to increased childhood illness, nutritional deficiencies and limited healthcare access, factors that are particularly relevant across Latin America, Brazil, Chile, and Mexico (Franco et al. 2024; Harz et al. 2023; Rai et al. 2018). However, the relationship between SEP and MIH is multifactorial and highly complex, with conflicting evidence across studies (Villanueva-Gutiérrez et al. 2019; Wuollet et al. 2018). The presence of siblings was identified as a protective factor against MIH in the present study, a finding that contrasts with research conducted in an Iraqi population, where a higher number of children in a family correlated with an increased prevalence of MIH (Ghanim et al. 2013). In the present study, the largest family had four children, with families of this size being infrequent. Conversely, in the Iraqi study, families had up to nine children, with four to six being the most common. In Mexico, family size has been decreasing over time, however, there is still an influence of SEP on family size, with families with lower socioeconomic income tending to have more children (Villasmil 2022). Family size in 1976 was reported to have an average of 4.8 members, in 1997, 3.1 and in 2006 it was reduced to 2.7 members (Menkes and Mojarro 2006), which may be the reason why the results of this study differ from those mentioned above in the Iraqi population.
The age of the participants was associated with higher prevalence of MIH, potentially due to the mean age being between 8 and 9 years, as this age range is important because most children have their four first permanent molars erupted. This is an optimal period for MIH screening and early diagnosis, limiting the amount of time that PEB and carious lesion development can occur in older cohorts, that may confound MIH diagnosis (Allazzam et al. 2014; Ghanim et al. 2011). Although the prevalence of MIH can increase or decrease depending on the year of birth (Koch et al. 1987), and as the aetiology of MIH is still uncertain, we cannot conclude there is a close relationship between age cohorts and MIH characteristics.
In the present study, bivariate analyses indicated a correlation trend, albeit statistically insignificant putatively due to the relatively small sample size, between childhood disease in the first three years-of-life and the use of antibiotics in the same period and MIH. The influence of early life health factors on MIH remains contentious. A 2022 meta-analysis by Garot and colleagues identified perinatal hypoxia, caesarean birth, and prematurity as major risks; postnatal conditions such as measles, otitis media, pneumonia, asthma and urinary tract infections were also associated with MIH (Garot et al. 2022). In Mexico, the caesarean birth rate is around 45% (Uribe-Leitz et al. 2019), significantly exceeding the 10—15% recommended by the World Health Organization (Organization 2021). In the present study, the prevalence was relatively lower at 34%; however, despite this high prevalence of caesarean deliveries there was not a statistically significant association between the mode of delivery and the presence of MIH, contrasting with a study of Garot and colleagues who reported a six-fold increase in MIH risk for infants with perinatal hypoxia and caesarean delivery (Garot et al. 2016). Moreover, in a retrospective parental questionnaire-based study of 1075 children from Medellin, Colombia, complications during the last trimester of pregnancy, low birth weight, respiratory problems, and urinary tract infections in the children were the factors most associated with MIH (Mejía et al. 2019).
In 2020, Lee and colleagues reported a relationship between MIH and maternal smoking during pregnancy and increased respiratory infections of the child in the first three years of life, putative causative factors for MIH (Lee et al. 2020). In the present study, only 1.4% of mothers reported smoking during pregnancy, and 30% of their children had MIH, a high prevalence but a very a small cohort that could be confounded by variables such as SES and reporting bias. The prevalence of smoking in Mexican women in urban areas is 18.4%, and there is a close relationship with high SES, and high SES in the present study was a protective factor for MIH, highlighting the potential for a confounding effect of multiple factors (Kuri-Morales et al. 2006; Ng et al. 2014; Ortiz-Hernández et al. 2015).
Current evidence suggests MIH results from a complex interplay of genetic, epigenetic and systemic factors, however, no single aetiological factor or group of factors has been conclusively identified (Garot et al. 2022). Retrospective studies, currently the dominant research model for investigations into aetiological studies of MIH, mostly rely on parental recall, which is prone to inaccuracy for events occurring at least six years prior. This is a limitation of the present study, as the search for an association between MIH presence and medical factors of the child or mother may have a high probability of recall bias. If data are sourced from health records, there is a possibility that the information collected is variable and not sufficient, lacking focus and consistency in recording data relevant to MIH. Meanwhile, longitudinal studies face high dropout rates and long-term feasibility challenges especially due to dropouts, with participants potentially being in the study from the last trimester of the mother’s pregnancy until the child is at least 6 years-of-age (for the eruption of FPMs and incisors) (Desai 2020). With MIH prevalence being high worldwide, its early diagnosis and management must be a priority in daily dental practice. The rates of hypersensitivity, enamel breakdown and early-stage caries in MIH patients underscores the importance of preventive strategies to improve outcomes. The present study contributes to the growing body of evidence highlighting MIH prevalence, clinical characteristics and risk factors, but many unanswered questions remain. Future research should focus on longitudinal studies with robust participant monitoring to ensure the highest level of accuracy. The challenges for MIH research and clinical management continue.




Comments (0)