HypoPT is a rare condition, most commonly occurring following total thyroidectomy or neck dissection for head and neck tumors. Due to its rarity, detailed knowledge about its treatment is typically confined to specialized medical circles. However, HypoPT patients are often treated by non-specialists, such as general practitioners, making it essential to communicate consensus-based expert knowledge on diagnosis, treatment, and monitoring to these providers.
We identified five areas of common support that can offer valuable guidance to non-specialists managing HypoPT: Consensus has been reached on the etiology of the primary cause, which laboratory values to measure, when, and what other procedures can be used to ensure the diagnosis, and on treatment and monitoring (including how to do it, what goals to achieve, when, and how to review goals). Although the existing German and international guidelines already make recommendations, some of these are not specifically formulated and differ with regard to certain statements (Table 4).
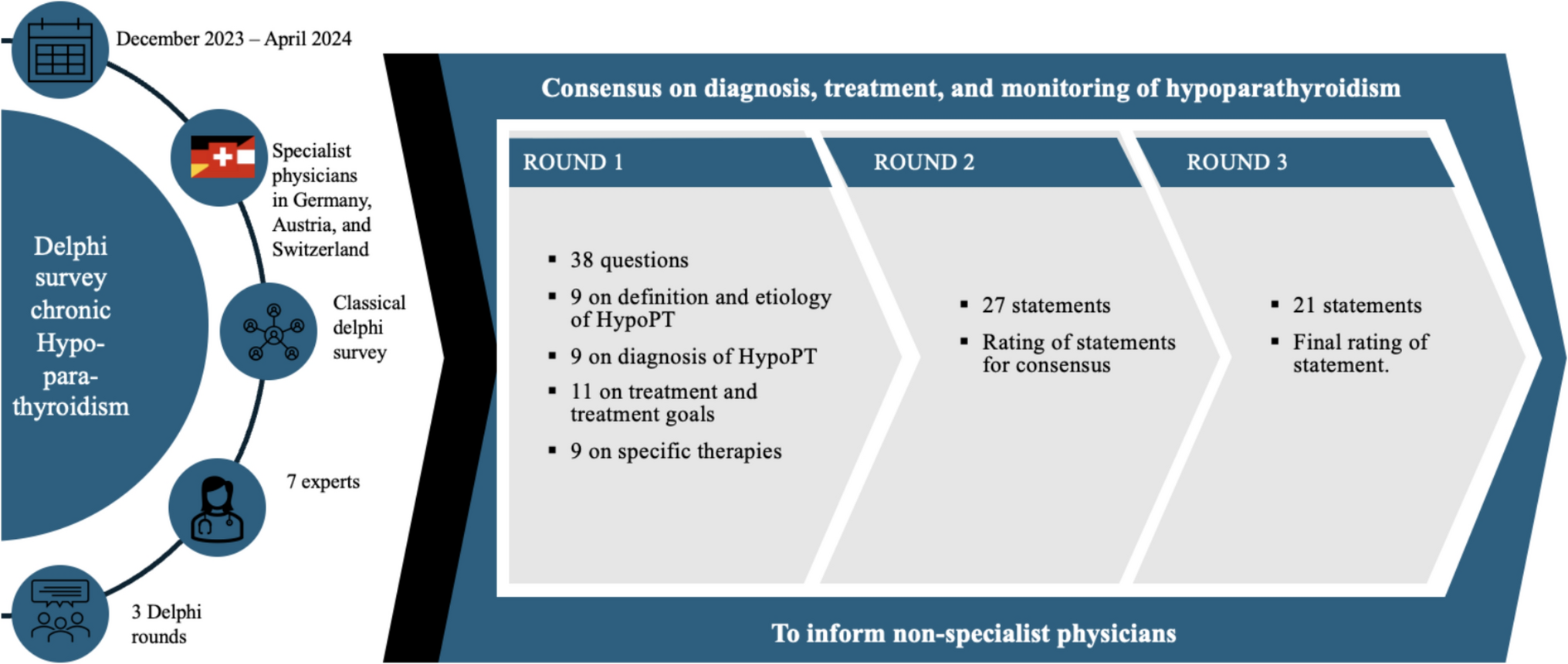
Table 4 Guideline recommendations and further clarifications in this Delphi surveyExperts in the DACH region estimate that at least 90% of all cases of HypoPT are of postoperative nature. This estimate is at the upper end of the interval reported in the literature [2, 17,18,19].
For the diagnosis of HypoPT, serum albumin-adjusted calcium measurement is performed within the first 24 postoperative hours according to guidelines [21, 22, 27]. Low serum calcium is defined as a subnormal albumin-adjusted total calcium of ≤ 8.4 mg/dL or ≤ 2.1 mmol/L [33]. Khan et al. add that in the case of hypocalcemia and undetectable/low serum PTH levels, the diagnosis should be confirmed by a second measurement at least 2 weeks apart [22]. In addition to the established measurement time within the first 24 postoperative hours, German-speaking experts agree that additional measurements of serum calcium within the first 2 postoperative weeks and then every 3 to 6 months should be used. Consequently, measurement of serum calcium more than 24 h postoperatively is still useful, especially in the presence of HypoPT-specific symptoms.
These symptoms can be complex and vary between patients. Paresthesia, muscle cramps and fatigue, nephrocalcinosis/nephrolithiasis, seizures, depression, ischemic heart disease, arrhythmias and, in the long term, cataracts and renal insufficiency are just some of them [12, 13, 34]. The experts in this Delphi survey concluded that paresthesia, muscle cramps, and fatigue are the three most common symptoms. The measurement of 24-h urine calcium and serum creatinine are part of the long-term monitoring of patients with chronic HypoPT recommended by most international guidelines and aim to capture long-term renal complications of chronic HypoPT (nephrocalcinosis/nephrolithiasis) [21].
Other monitoring examinations such as kidney ultrasound, bone mineral density measurements and cranial CT scans are optional with higher significance in long-term disease and monitoring.
In addition to serum albumin-adjusted calcium, the measurement of serum PTH levels is the second key biochemical parameter for the diagnosis of HypoPT. There is a consensus in published guidelines and in our Delphi survey that a low serum PTH level is key for the diagnosis HypoPT. However, a defined threshold for a low serum PTH level of < 10 pg/mL in the immediate post-operative period is reported only by Khan et al. [22]. The Position Statement of the PARAT program identified an additional approach, namely calculating the ratio between pre- and post-surgical serum PTH concentrations and the decrease of > 70% as being strongly associated with chronic Hypo-PT [21].
The main problem in establishing serum PTH threshold levels is the use of different generations of immunoassays that result in different normal ranges of serum PTH concentrations [2]. This is supported by the meta-analysis of Nagel et al. [31]. Therein, 40 different PTH assays deriving from 81 studies were cited to avoid assay-related confusion in preoperative serum PTH and calcium measurements. They suggest that both serum PTH and albumin-adjusted calcium levels should be measured by the same laboratory where the initial postoperative measurements were performed [31]. For the diagnosis of HypoPT, the overall clinical manifestations in combination with low serum albumin-adjusted calcium and low serum PTH levels are more important diagnostic criteria for HypoPT than an isolated PTH value below a pre-defined threshold.
With regards to monitoring, a regular measurement of 24-h urine calcium and serum creatinine levels is widely used. Our experts agree that these parameters should be assessed once a year. Khan et al. [22] support a range of 6–24 months and Bollerslev et al. [21] recommend creatinine measurement every 3–6 months. In any case, measurement of the above values should be performed in a regular context within the specified period. Therefore, the results of this Delphi survey provide an operationalized guidance for these monitoring parameters.
Health-related quality of life is a key goal of treatment and monitoring. As this aspect is not reflected by biochemical measurements, further reference points are needed. The experts in this Delphi survey therefore unanimously agree on the importance of usage of standardized questionnaires specifically designed for HypoPT. While Bollerslev et al. [21] do not mention instruments to measure quality of life, Khan et al. [22] refer to monitoring using the standardized and validated “SF-36” [4] developed for chronic diseases and the “Hypoparathyroidism Patient Experience Scale (HPES) is a psychometrically validated, disease-specific measure specifically designed to assess the symptoms and impacts associated with hypoparathyroidism [32]. The SF-36 questionnaire, which was not explicitly developed for the HypoPT, is the most commonly used instrument for measuring quality of life in the literature [35]. Three HypoPT-specific questionnaires have been developed, the Hypoparathyroidism Symptom Diary [36], the [Hypoparathyroidism Patient Experience Scale (HPES) [32, 37], and the German disease-specific questionnaire HPQ28] [38,39,40,41]. Only the HPQ28 has been prospectively tested in HypoPT patients, validated compared to disease-specific control groups and the normal population and is available free of cost. The use of these specific questionnaires as part of the monitoring program of patients with chronic HypoPT, i.e., every 6–12 months, is recommended if possible.
No recommendations for possible PTH replacement therapies were included in the German postoperative guideline from 2021 [27]. Evaluation of PTH therapy is generally recommended for patients who are not well controlled on calcium and active vitamin D treatment. In the European Union, only two PTH therapies have been approved for the treatment of chronic HypoPT in adults (none in children). The first was a once-daily injection of rhPTH(1–84). As production ended in 2024, this treatment is no longer available [42]. The second is palopegteriparatide (or TransCon PTH), which is available as a once-daily injection. Palopegteriparatide is a prodrug of PTH(1–34), administered once-daily, designed to provide active PTH within the physiologic range for 24 h/day [43]. The primary goal of PTH-replacement therapy with palopegteriparatide is to maintain serum calcium within the normal range without need for additional treatment with active vitamin D and oral calcium beyond low doses (calcium dose ≤ 600 mg/d) [44]. This form of therapy therefore has the chance to significantly reduce daily pill burden of calcium and vitamin D, identified as one important factor decreasing quality of life in HypoPT patients [35, 45]
In the PaTHway study, independence from calcium and active vitamin D supplements was achieved in 79% of all participants receiving palopegteriparatide, and mean 24-h urine calcium was normalized. Furthermore, a significant treatment effect on wellbeing was seen, measured with the hypoparathyroidism patient experience scale (HPES) and 36-Item Short Form Survey (SF-36) [44]. When treating HypoPT with PTH replacement therapy, experts agree that therapy should be monitored quarterly after a stable dose is reached.
International guidelines agree on the use of PTH replacement therapy in selected patients who are not adequately controlled on therapy with calcium and active vitamin D supplementation. Khan et al. [22] recommend PTH replacement therapy in patients with symptomatic hypocalcemia, hyperphosphatemia, renal insufficiency, hypercalciuria, or poor quality of life. Bollerslev et al. [21] suggest PTH therapy for patients whose serum and urine calcium cannot be kept within target ranges in a stable and safe manner. Furthermore, serum albumin-adjusted calcium levels that are persistently outside the normal range and hypercalciuria are additional indications for PTH replacement therapy.
They also specify that PTH replacement therapy should be initiated in the event of persistent symptoms and/or the need for hospitalization, as well as in cases of poor tolerance of treatment with calcium and active vitamin D. This indicates that factors beyond biochemical parameters play a role in the response to treatment. This Delphi survey was conducted before and during the early phases of market entry of palopegteriparatide, therefore no wide spread experience with its usage in the German market existed during the time of this project.
While this Delphi survey provides valuable guidance from experts on HypoPT, there are several limitations to consider. First, the small sample size of seven clinical experts limits the generalizability of the findings. Although this number is consistent with the Delphi method, a larger panel might capture a broader spectrum of clinical opinions and practices.
Second, although we identified and reached consensus on many relevant factors for HypoPT diagnosis, treatment, and monitoring, this list is not exhaustive. Additional parameters and factors may be required in clinical practice depending on patient-specific needs and evolving treatment protocols. Future research should explore these additional parameters and validate them within broader patient populations to further enhance practical applicability.
Furthermore, while consensus was reached on many diagnostic and monitoring practices, areas such as the exact threshold for PTH levels and the optimal timing for identifying chronic HypoPT were less conclusive. This ambiguity highlights the ongoing need for research and further refinement of best practices for HypoPT management.
Lastly, while consensus was achieved on the importance of quality of life measurements, there is currently no universally accepted disease-specific tool for HypoPT in clinical practice. The HPQ28 questionnaire offers a promising approach being available in German and free of cost and should be progressively implemented in the regular care of HypoPT patients in future. Having been originally been drafted in German and English, it is now also available in other languages. In particular, it has been adapted and validated in French and Danish, while adaptations in Italian, Czech, Spanish and Turkish are pending. The still existing gap in QOL documentation underscores the importance of continued validation and implementation of such tools to better support patient-centered care in everyday clinical practice.




Comments (0)